

Characterization and Clinical Implications of p53 Dysfunction in Patients With Myelodysplastic Syndromes
- PMID: 40315418
- PMCID: PMC12169866
- DOI: 10.1200/JCO-24-02394
Characterization and Clinical Implications of p53 Dysfunction in Patients With Myelodysplastic Syndromes
Abstract
Purpose: Tumor Protein 53 (p53) expressed from gene TP53 is a seminal tumor suppressor. We aimed to characterize mutational and nonmutational mechanisms of p53 dysfunction in myelodysplastic syndromes (MDS) and to investigate their clinical effect.
Patients and methods: We analyzed a cohort of 6,204 patients with MDS and subsets of patients with available information on RNA sequencing of tumor cells (n = 109), high-dimensional phenotype of immune cells (n = 77), and multiomics analysis (RNA sequencing and proteomics) on single cells (n = 15). An independent validation was performed on 914 patients.
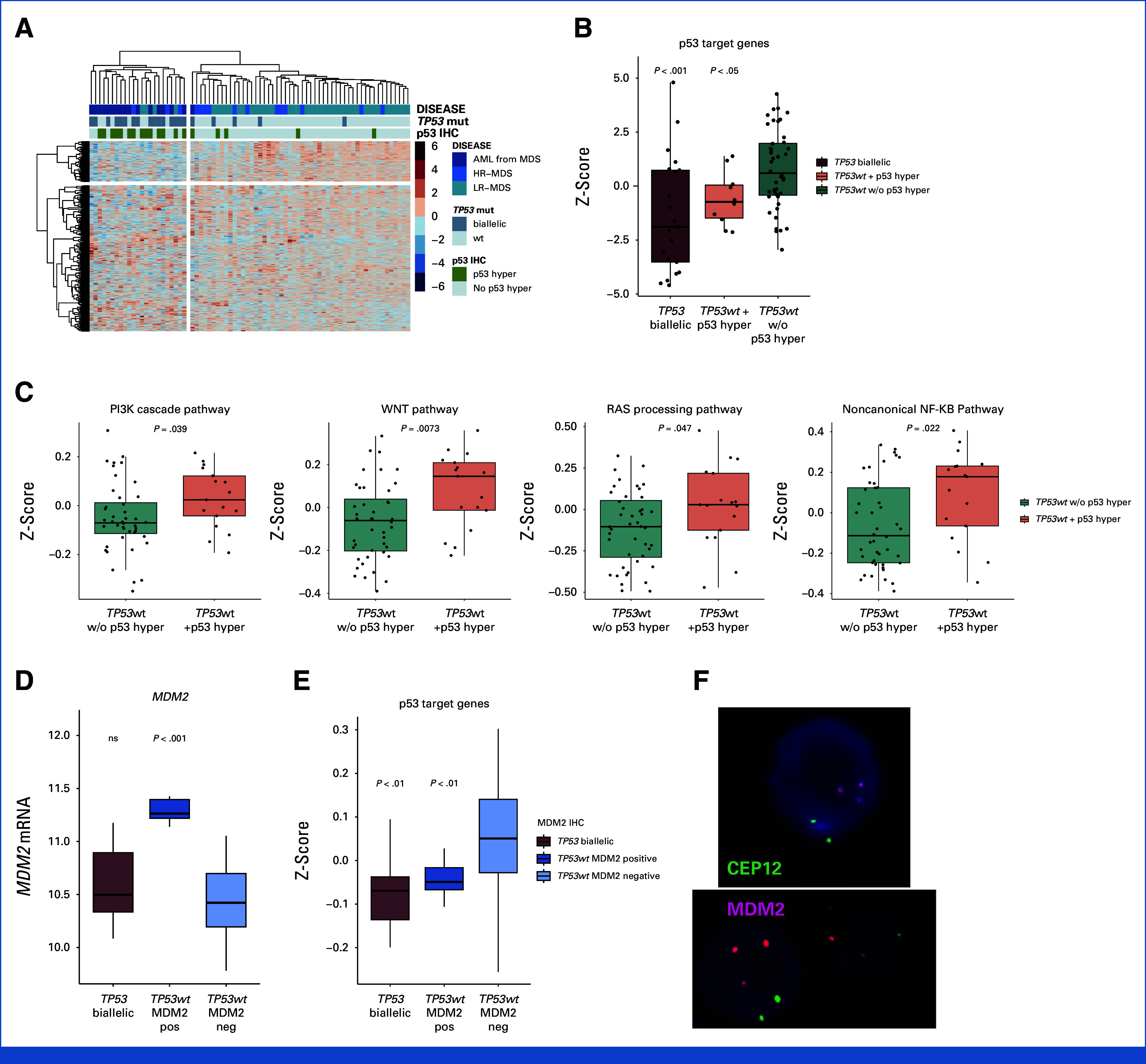
Results: Biallelic TP53 inactivation was a powerful driver of disease progression and identified high-risk patients, regardless of variant allele frequency. Monoallelic and biallelic inactivation represent disease stages occurring as a multihit process in MDS with TP53 mutations, thus potentially refining the optimal timing of therapeutic interventions in these patients. We identified a subset of MDS (5%) characterized by TP53 wild-type and hyperexpression of abnormal p53 protein in bone marrow progenitors that exhibit dismal outcome. These patients presented upstream p53 signaling aberrations in Pi3K cascade; RAS, WNT, and NF-KB pathways; and MDM2 gene amplification, together with a downstream dysregulation of p53 targets. MDS with p53 dysfunction displayed a distinct immune dysregulation involving myeloid-derived inflammation and impaired antigen presentation, which may be a driver of their poor prognosis and provide the groundwork for innovative immunotherapies.
Conclusion: The identification of nonmutational p53 dysfunction in MDS may lay the foundation for a mechanistic classification of myeloid neoplasms, moving beyond a purely molecular stratification. The recognition of patients with p53 dysfunction is relevant to provide correct disease-risk assessment and interventions, as well as to refine the design of clinical trials.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures




References
-
- Vousden KH, Lane DP. p53 in health and disease. Nat Rev Mol Cell Biol. 2007;8:275–283. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
