

An artificial intelligence interpretable tool to predict risk of deep vein thrombosis after endovenous thermal ablation
- PMID: 40316015
- PMCID: PMC12175713
- DOI: 10.1016/j.jvsv.2025.102253
An artificial intelligence interpretable tool to predict risk of deep vein thrombosis after endovenous thermal ablation
Abstract
Objective: Endovenous thermal ablation (EVTA) stands as one of the primary treatments for superficial venous insufficiency. Concern exists about the potential for thromboembolic complications following this procedure. Although rare, those complications can be severe, necessitating early identification of patients prone to increased thrombotic risks. This study aims to leverage artificial intelligence-based algorithms to forecast patients' likelihood of developing deep vein thrombosis (DVT) within 30 days following EVTA.
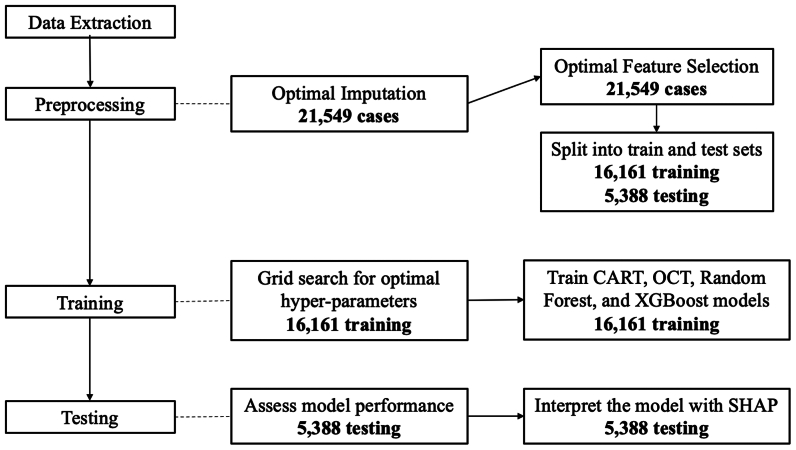
Methods: From 2007 to 2017, all patients who underwent EVTA were identified using the American College of Surgeons National Surgical Quality Improvement Program database. We developed and validated four machine learning models using demographics, comorbidities, and laboratory values to predict the risk of postoperative DVT: Classification and Regression Trees (CART), Optimal Classification Trees (OCT), Random Forests, and Extreme Gradient Boosting (XGBoost). The models were trained using all the available variables. SHapley Additive exPlanations analysis was adopted to interpret model outcomes and offer medical insights into feature importance and interactions.
Results: A total of 21,549 patients were included (mean age, 54 ± 14 years; 67% female). In this cohort, 1.59% developed DVT. The XGBoost model had good discriminative power for predicting DVT risk with area under the curve of 0.711 in the hold-out test set for the all-variable model. Stratification of the test set by age, body mass index, preoperative white blood cell count, and platelet count shows that the model performs equally well across these groups.
Conclusions: We developed and validated an interpretable model that enables physicians to predict which patients with superficial venous insufficiency has higher risk of developing DVT within 30 days following EVTA.
Keywords: Artificial intelligence; Chronic venous disease; Endovascular thermal ablation; Radiofrequency ablation; Superficial venous disease; Venous stripping.
Copyright © 2025 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures None.
Figures




References
-
- Nellis J.M., Obi A.T., Powell C.A., Wakefield T.W. Treatment and contemporary outcomes associated with adjunct tourniquet use during phlebectomy of complex, voluminous truncular varicosities. J Vasc Surg Venous Lymphat Disord. 2022;10:1208–1214. - PubMed
-
- Fletcher S.E., Jasuja S., Lawler L.P., Moriarty J.M. Catheter directed thrombolysis and mechanical intervention in deep venous thrombosis: what is the status after the ATTRACT Trial? Postgrad Med. 2021;133:42–50. - PubMed
-
- Kakkos S.K., Gohel M., Baekgaard N., et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2021 clinical practice guidelines on the management of venous thrombosis. Eur J Vasc Endovasc Surg. 2021;61:9–82. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
