

Prospective study on ultrasonographic measurement of the spinal canal depth in very low birth weight infants
- PMID: 40316404
- PMCID: PMC12049973
- DOI: 10.1136/bmjpo-2024-003079
Prospective study on ultrasonographic measurement of the spinal canal depth in very low birth weight infants
Abstract
Background: Lumbar punctures (LP) in very low birth weight (VLBW) infants often have low success rates. Point-of-care ultrasound (POCUS)-based spinal canal depth (SCD) measurements may provide better outcomes.
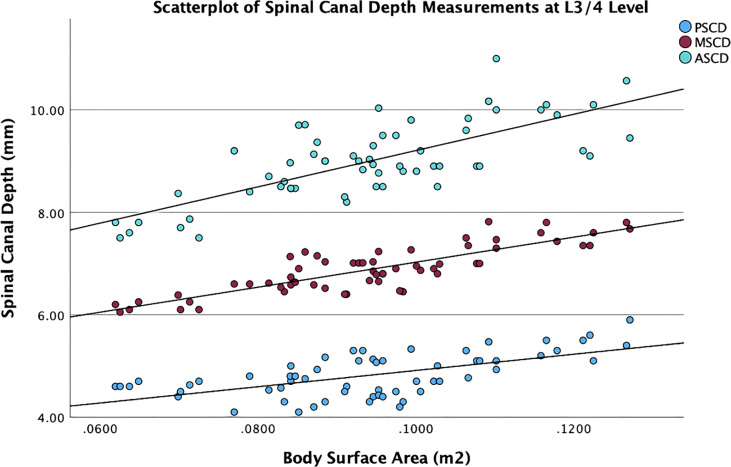
Aim: To provide POCUS-based SCD measurement values for VLBW infants using different calculation methods at the L4/5 and L3/4 levels.
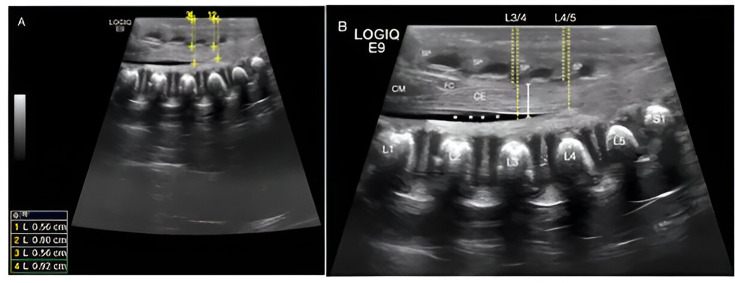
Methods: This prospective observational study involved 31 VLBW infants in the neonatal intensive care unit at Women's Wellness and Research Center, Doha, Qatar, from March 2022 to September 2023. The outcome measures included anterior (ASCD), mid (MSCD) and posterior spinal canal depth (PSCD) measurements. The study compared results from different calculation methods at the L4/5 and L3/4 levels.
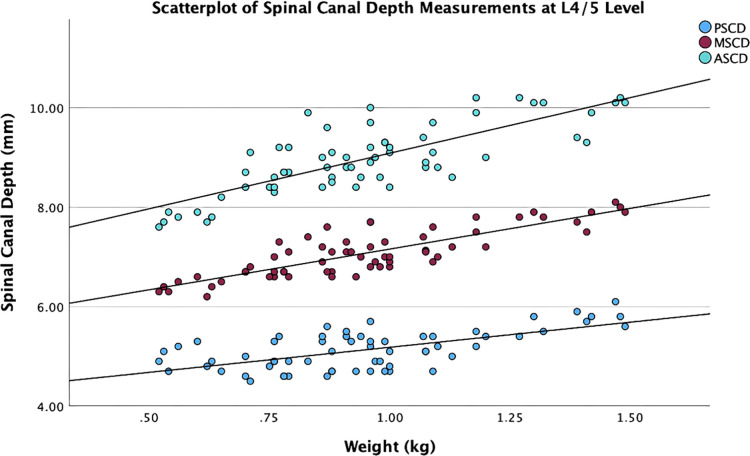
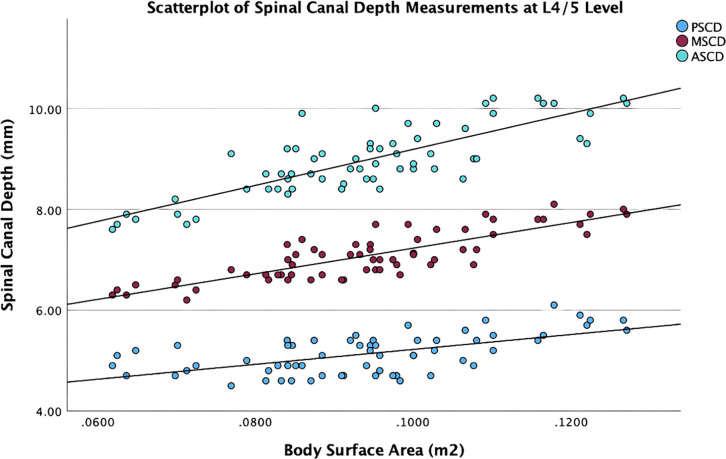
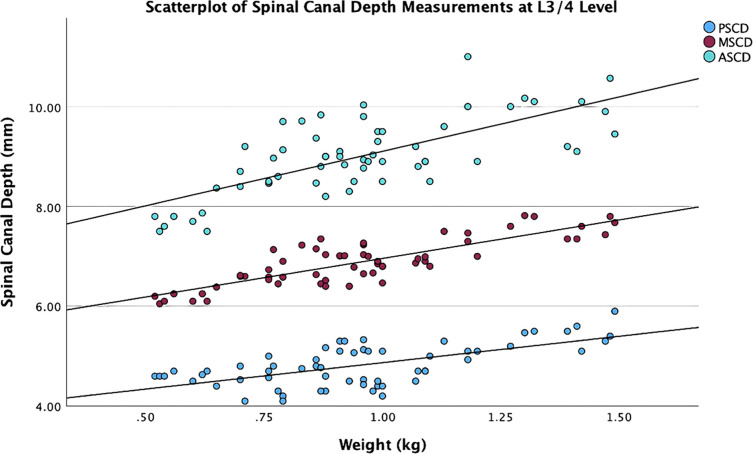
Results: A total of 63 ultrasound examinations were performed on 31 infants. The median gestational age was 25.0 weeks (IQR 24-27), with a birth weight of 817.9±170.2 g and a birth height of 31.6±2.8 cm. The MSCD at L4/5 was 7.1±0.5 mm and 6.9±0.5 mm at L3/4, with a mean difference (MD) of 0.20 (95% CI 0.15 to 0.24; p<0.001). The mean SC anteroposterior diameter at L4/5 was 3.8 mm versus 4.2 mm at L3/4 (MD -0.334, 95% CI -0.45 to 0.22; p<0.001). Weight-based and body surface area (BSA) calculations correlated best with MSCD at both levels. The MSCD in millimetres was determined by the equations 2×weight (kg)+6 (R²=0.71) at L4/5 and (R²=0.70) at L3/4 and 25×BSA (m²)+5 (R²=0.71) at L4/5 and (R²=0.73) at L3/4 levels. Moreover, body weight and BSA showed a slightly stronger correlation with ASCD measurements compared with PSCD. All SCD measurements demonstrated a poor linear correlation with body length (cm) and body mass index (kg/m²).
Conclusion: This study offers reference data for POCUS-based SCD measurements in VLBW infants, demonstrating that body weight and BSA effectively predict SCD. These findings could enhance the accuracy of LPs in this population when ultrasound guidance is unavailable, supporting personalised care.
Keywords: Data Collection; Infant; Neonatology; Qualitative research; Technology.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Ultrasonographic determination of neonatal spinal canal depth.Arch Dis Child Fetal Neonatal Ed. 2008 Nov;93(6):F451-4. doi: 10.1136/adc.2007.129221. Epub 2008 Feb 19. Arch Dis Child Fetal Neonatal Ed. 2008. PMID: 18285380
-
MR determination of neonatal spinal canal depth.Eur J Radiol. 2012 Aug;81(8):e813-6. doi: 10.1016/j.ejrad.2012.02.003. Epub 2012 May 18. Eur J Radiol. 2012. PMID: 22609321
-
Weight-based determination of spinal canal depth for paediatric lumbar punctures.Arch Dis Child. 2013 Nov;98(11):877-80. doi: 10.1136/archdischild-2013-303793. Epub 2013 Aug 21. Arch Dis Child. 2013. PMID: 23966025
-
Visceral adiposity and inflammatory bowel disease.Int J Colorectal Dis. 2021 Nov;36(11):2305-2319. doi: 10.1007/s00384-021-03968-w. Epub 2021 Jun 9. Int J Colorectal Dis. 2021. PMID: 34104989 Review.
-
Sound reduction management in the neonatal intensive care unit for preterm or very low birth weight infants.Cochrane Database Syst Rev. 2020 Jan 27;1(1):CD010333. doi: 10.1002/14651858.CD010333.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2024 May 30;5:CD010333. doi: 10.1002/14651858.CD010333.pub4. PMID: 31986231 Free PMC article. Updated.
References
-
- Pinheiro JM, Furdon S, Ochoa LF. Role of local anesthesia during lumbar puncture in neonates. Pediatrics. 1993;91:379–82. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources