

Diagnostic dilemma of a new endobronchial lesion in a patient on anti-tuberculosis regimen: unveiling tuberculosis immune reconstitution inflammatory syndrome
- PMID: 40316898
- PMCID: PMC12048918
- DOI: 10.1186/s12879-025-11047-6
Diagnostic dilemma of a new endobronchial lesion in a patient on anti-tuberculosis regimen: unveiling tuberculosis immune reconstitution inflammatory syndrome
Abstract
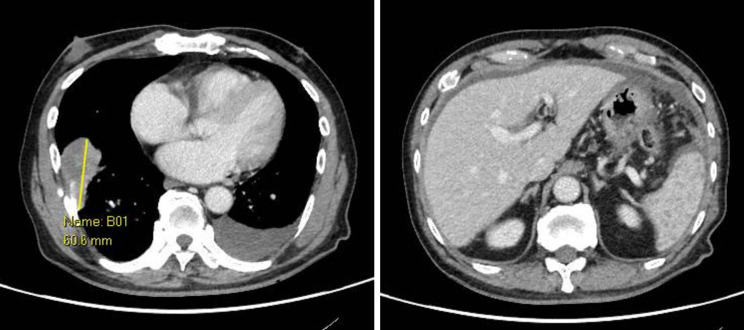
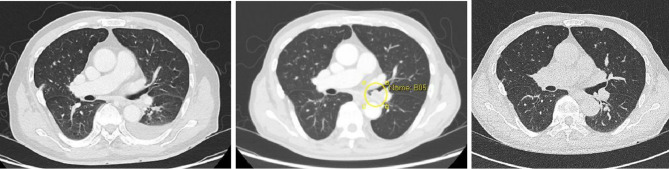
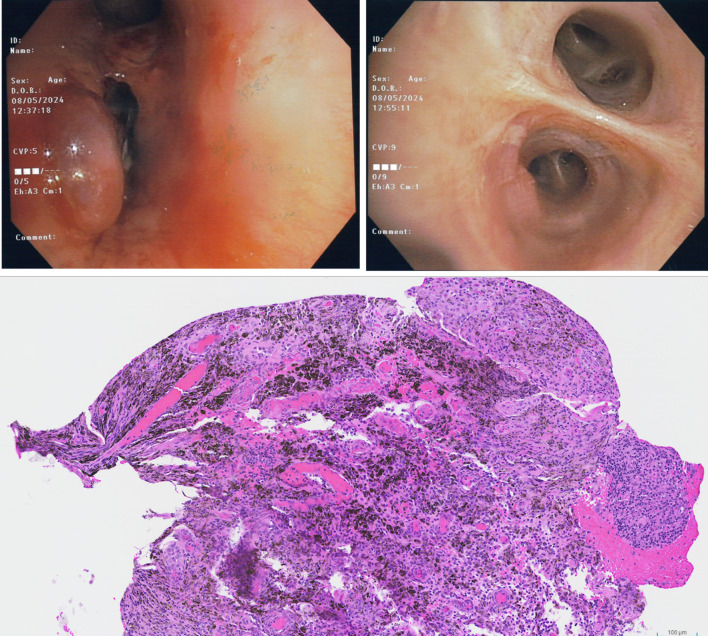
A 76-year-old gentleman with chronic plaque psoriasis was found to have a right lower lobe mass with bilateral pulmonary nodules, extensive lymphadenopathy, splenic hypodensities and diffuse peritoneal thickening on the computed tomography (CT) scan 5 months after initiation of adalimumab. Biopsies of the RLL mass and supraclavicular lymph node showed granulomatous inflammation and cultures were positive for Mycobacterium tuberculosis (MTB). Adalimumab was stopped and he was started on TB treatment. He remained well and asymptomatic but was noted to have 3 kg weight loss. Interval CT scan 3 months later showed enlarging mediastinal lymph nodes confluent with a new left lower lobe endobronchial mass. Sputum, bronchoalveolar lavage and bronchial biopsy samples were negative for evidence of active TB. Histology showed granulation tissue with both acute and chronic inflammation. Diagnostic impression was asymptomatic TB immune reconstitution inflammatory syndrome (IRIS), and he was maintained on the existing TB treatment. Interval CT 1 month later showed resolution of the endobronchial mass. In patients without human-immunodeficiency virus (HIV) infection, IRIS after initiation of TB treatment is rare. Without standardised diagnostic criteria, TB IRIS can be challenging to diagnose especially in absence of clinical symptoms. Patients with TB IRIS can have serious complications but may also be asymptomatic with only radiological abnormalities. Hence a high clinical suspicion is needed for the diagnosis, especially in patients presenting initially with disseminated disease or with underlying immune dysregulation such as in this patient who had been on anti- TNF-α treatment. Exclusion of alternative diagnoses is important. Our case also highlights the importance of a personalised approach (with combination tests) especially among immunosuppressed patients with prior TB disease.
Not applicable.
Keywords: TB immune reconstitution inflammatory syndrome; TNF alpha antagonists.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: SingHealth Centralised Institutional Review Board (CIRB) review was not required for case report of one to two patients. Consent for publication: Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. Competing interests: The authors declare no competing interests.
Figures
References
-
- Bagcchi S. WHO’s global tuberculosis report 2022. Lancet Microbe. 2023;4(1):e20. - PubMed
-
- Wallis RS. Reactivation of latent tuberculosis by TNF Blockade: the role of interferon γ. J Invest Dermatology Symp Proc. 2007;12(1):16–21. - PubMed
-
- Kasiraman V, Atwan AA, Durojaiye OC, Kalavala M, Piguet V. Risk of tuberculosis with the use of anti-TNF medications in psoriasis: incidence, screening and management. Dermatol Online J. 2014;20(8). - PubMed
-
- Namale PE, Abdullahi LH, Fine S, Kamkuemah M, Wilkinson RJ, Meintjes G. Paradoxical TB-IRIS in HIV-infected adults: a systematic review and Meta-analysis. Future Microbiol. 2015;10(6):1077–99. - PubMed
-
- Sueki H, Mizukawa Y, Aoyama Y. Immune reconstitution inflammatory syndrome in non-HIV immunosuppressed patients. J Dermatol. 2018;45(1):3–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
