

The urea-to-creatinine ratio as an emerging biomarker in critical care: a scoping review and meta-analysis
- PMID: 40317012
- PMCID: PMC12046807
- DOI: 10.1186/s13054-025-05396-6
The urea-to-creatinine ratio as an emerging biomarker in critical care: a scoping review and meta-analysis
Abstract
Background: Severe protein catabolism is a major aspect of critical illness and leads to pronounced muscle wasting and, consequently, extended intensive care unit (ICU) stay and increased mortality. The urea-to-creatinine ratio (UCR) has emerged as a promising biomarker for assessing protein catabolism in critical illness, which is currently lacking. This review aims to elucidate the role of UCR in the context of critical illness.
Methods: This scoping review adhered to the PRISMA Extension for Scoping Reviews guidelines. A comprehensive literature search was conducted on the 3rd of September 2024, across Embase, PubMed, ScienceDirect, and Cochrane Library to identify studies related to (1) critically ill adult patients and (2) reporting at least a single UCR value. A meta-analysis was conducted for ≥ 5 studies with identical outcome parameters.
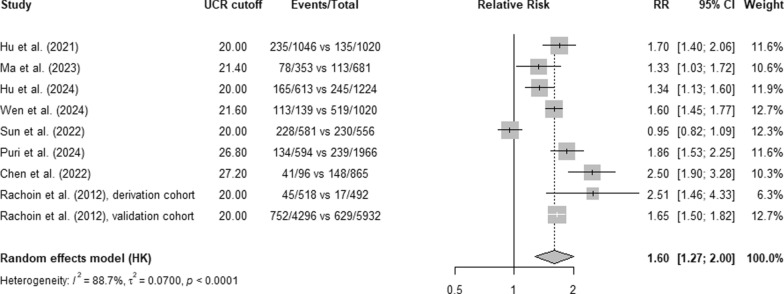
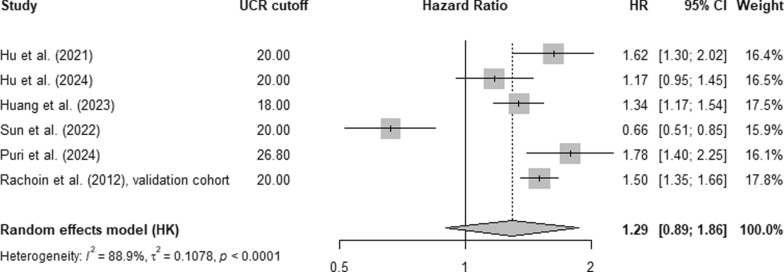
Results: Out of 1,450 studies retrieved, 47 were included in this review, focusing on UCR's relation to protein catabolism and persistent critical illness (10 studies), mortality (16 studies), dietary protein interventions (2 studies), and other outcomes (19 studies), such as delirium, and neurological and cardiac adverse events. UCR is inversely correlated to muscle cross-sectional area over time and associated to length of ICU stay, emphasising its potential role in identifying patients with ongoing protein catabolism. A UCR (BUN-to-creatinine in mg/dL) of ≥ 20 (equivalent to a urea-to-creatinine in mmol/L of approximately 80) upon ICU admission, in comparison with a value < 20, was associated with a relative risk of 1.60 (95% CI 1.27-2.00) and an adjusted hazard ratio of 1.29 (95% CI 0.89-1.86) for in-hospital mortality.
Discussion: UCR elevations during critical illness potentially indicate muscle protein catabolism and the progression to persistent critical illness, and high levels at ICU admission could be associated with mortality. UCR increments during ICU stay may also indicate excessive exogenous dietary protein intake, overwhelming the body's ability to use it for whole-body or muscle protein synthesis. Dehydration, gastrointestinal bleeding, kidney and liver dysfunction, and renal replacement therapy may also influence UCR and are considered potential pitfalls when assessing catabolic phases of critical illness by UCR. Patient group-specific cut-off values are warranted to ensure its validity and application in clinical practice.
Keywords: Critical illness; Intensive care unit; Nutrition; Protein catabolism; UCR; Urea-to-creatinine ratio.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Conflict of interest: The authors declare no competing interests.
Figures


Comment in
-
Reconsidering the urea-to-creatinine ratio as a signal of muscle catabolism in patients with cirrhosis.Crit Care. 2025 Oct 8;29(1):428. doi: 10.1186/s13054-025-05703-1. Crit Care. 2025. PMID: 41063279 Free PMC article. No abstract available.
References
-
- Puthucheary ZA, Rawal J, McPhail M, Connolly B, Ratnayake G, Chan P, et al. Acute skeletal muscle wasting in critical illness. JAMA. 2013;310(15):1591–600. - PubMed
-
- Darvall JN, Boonstra T, Norman J, Murphy D, Bailey M, Iwashyna TJ, et al. Persistent critical illness: baseline characteristics, intensive care course, and cause of death. Crit Care Resusc. 2019;21(2):110–8. - PubMed
-
- Iwashyna TJ, Hodgson CL, Pilcher D, Bailey M, van Lint A, Chavan S, et al. Timing of onset and burden of persistent critical illness in Australia and New Zealand: a retrospective, population-based, observational study. Lancet Respir Med. 2016;4(7):566–73. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
