

National trends in patient characteristics, interventional techniques and outcomes of endovascular treatment for acute ischaemic stroke: Final results of the MR CLEAN Registry (2014-2018)
- PMID: 40317163
- PMCID: PMC12049364
- DOI: 10.1177/23969873251334271
National trends in patient characteristics, interventional techniques and outcomes of endovascular treatment for acute ischaemic stroke: Final results of the MR CLEAN Registry (2014-2018)
Abstract
Introduction: Endovascular thrombectomy (EVT) procedures and workflow have evolved over the years. We examined trends in patient characteristics, EVT techniques and outcomes over 5 years in the Netherlands.
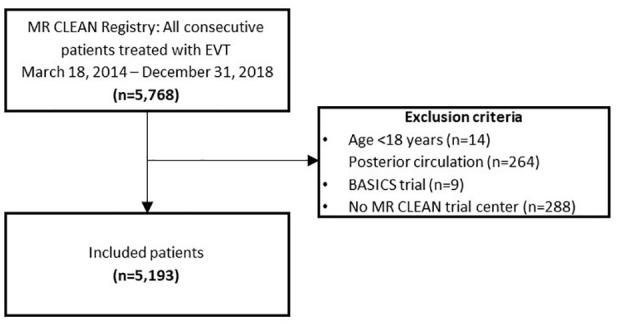
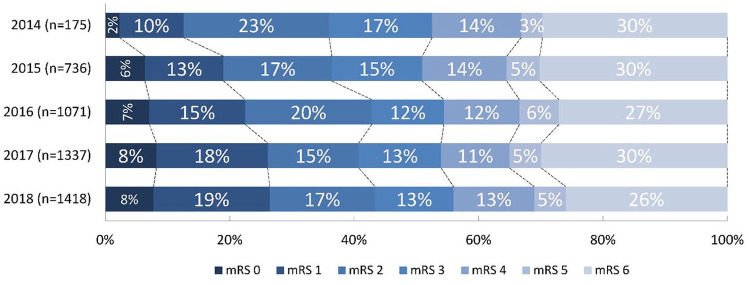
Patients and methods: Data from the MR CLEAN Registry (2014-2018) were analysed, including patients treated with EVT for anterior circulation acute ischaemic stroke (AIS). Patients were grouped by year of inclusion except for the linear regression analysis where the inclusion date was used. Baseline predicted probability of poor outcome (modified Rankin Scale (mRS) score 3-6) was calculated using a validated prediction model. Primary outcome was mRS score at 90 days. Secondary outcomes included workflow times, EVT techniques, successful reperfusion (eTICI ⩾ 2B) and symptomatic intracranial haemorrhage (sICH). Time trends were analysed using multivariable regression models (adjusted common odds ratios (acOR) per year).
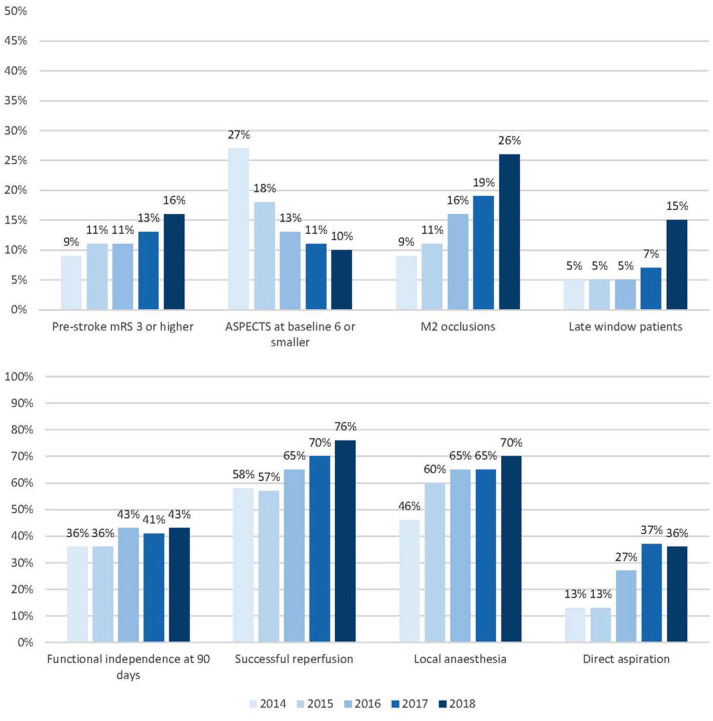
Results: 5193 patients were included. Median age increased (from 66 in 2014 to 74 years in 2018 [p < 0.001]). Proportion of patients with pre-stroke dependence (mRS ⩾ 3) increased from 2014 through 2018 (9% to 16%, p < 0.001). Baseline predicted probability of poor outcome did not change (60% vs 66%, p = 0.06). Over time, functional outcomes improved (acOR 1.14 per year, 95%CI: 1.09-1.20); mortality decreased (aOR 0.88 per year, 95%CI: 0.83-0.94). EVT under local anaesthesia increased (from 46% in 2014 to 70% in 2018; aOR 1.15, 95%CI: 1.10-1.22), as did use of direct aspiration (13%-36%; aOR 1.43, 95%CI: 1.35-1.53). Successful reperfusion became more frequent (aOR 1.32 per year, 95%CI: 1.25-1.40), despite needing more attempts (1 in 2014 vs 2 in 2018, aOR 0.93 per year, 95%CI: 0.89-0.98). Incidence of sICH remained unchanged (5% vs 5%, aOR 0.99 per year, 95%CI: 0.89-1.09). Time from emergency room to groin puncture reduced by 7 min per year (95%CI: 5-8).
Discussion and conclusion: Enhanced workflow and increased EVT experience may have led to shorter time to treatment and more frequent successful reperfusion, with better functional outcomes over 5 years, despite treating older, more dependent patients.
Keywords: MR CLEAN; acute ischaemic stroke; endovascular treatment; interventional techniques; large vessel occlusion; patient characteristics; registry; reperfusion; stroke.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Bokkers received unrestricted grants from the Netherlands Organization for Health Research and Development, the Dutch Ministry of Economic Affairs and Climate Policy and Siemens Healthineers. He received consulting fees from Guerbet which were paid to institution. Dr Uyttenboogaart received grants from the Dutch Heart Foundation, and TKI-PPS, paid to institution. Dr Boogaarts received a consulting fee from Stryker Neurovascular, paid to institution. Dr Postma received grants from Siemens Healthineers and Bayer Healthcare, paid to institution. Dr Yoo received grants from Medtronic, Ceronovus, Penumbra, Stryker and Genentech, paid to institution, and personal fees from Cerenovus, Penumbra, Vesalio, not related to the submitted work. He has equity ownership interest from Insera Therapeutics. Dr van der Lugt received grants from Stryker, Penumbra, Medtronic, Cerenovus, Thrombolytic Science LLC, Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organisation for Health Research and Development, Health Holland Top Sector Life Sciences & Health, GE Healthcare, Siemens Healthineers, Philips Healthcare, all paid to institution. He is on the DSMB of Escape-MEVO and is research leader of the CONTRAST consortium (unpaid). Dr van der Worp received grants from Stryker, Dutch Hearth Foundation, European Commission. He received consulting fees for TargED and Bayer. He is member of the executive committee of European Stroke Organisation. He has a stock in Philips. Dr Wermer is on the DSMB of the Trident trial. Dr Majoie received grants from CVON/Dutch Heart Foundation, Stryker, European Commission, TWIN, Dutch Health Evaluation Program and is shareholder of Nico.Lab. Dr Dippel received grants from Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organisation for Health Research and Development, Health Holland Top Sector Life Sciences & Health, Stryker, Penumbra, Inc, Medtronic, Thrombolytic Science LLC, Cerenovus. Dr Coutinho received grants from Boehringer Ingelheim, Bayer, Portola, outside the submitted work. Dr van Doormaal is on the advisory board of Diagnostix.ai and is shareholder of Diagnostix.ai. Dr van Zwam received payment to institution for unrelated consultancy activities for Stryker, Cerenovus, Medtronic, Penumbra, Microvention and Nico.Lab, and chairs the DSMBs of WE-TRUST (Philips, paid to institution), In Extremis (CHU Montpellier, unpaid) and ANAIS (Anaconda, paid to institution) studies. Dr R. van den Berg received payment to institution for unrelated consultancy activities for Cerenovus. Dr van Oostenbrugge is on the scientific advisory board (DSMB) of CoreValve Advance Study (MedTronic). Dr Roos and Ivo Jansen are shareholder at Nico.Lab. Dr Emmer received grants from Leading the Change Program (the Netherlands Organisation for Health Research and Development) and grants from Health Holland Top Sector Life Sciences & Health, outside the submitted work and paid to institution. The other authors report no conflicts.
Figures
Similar articles
-
Benefit of successful reperfusion achieved by endovascular thrombectomy for patients with ischemic stroke and moderate pre-stroke disability (mRS 3): results from the MR CLEAN Registry.J Neurointerv Surg. 2023 May;15(5):433-438. doi: 10.1136/neurintsurg-2022-018853. Epub 2022 Apr 12. J Neurointerv Surg. 2023. PMID: 35414601 Clinical Trial.
-
Clinical Outcome After Endovascular Treatment in Patients With Active Cancer and Ischemic Stroke: A MR CLEAN Registry Substudy.Neurology. 2022 Mar 8;98(10):e993-e1001. doi: 10.1212/WNL.0000000000013316. Epub 2022 Jan 11. Neurology. 2022. PMID: 35017306 Clinical Trial.
-
Admission blood pressure and clinical outcomes in patients with acute ischaemic stroke treated with intravenous alteplase and endovascular treatment versus endovascular treatment alone: A MR CLEAN-NO IV substudy.Eur Stroke J. 2023 Sep;8(3):647-654. doi: 10.1177/23969873231173274. Epub 2023 May 11. Eur Stroke J. 2023. PMID: 37641554 Free PMC article. Clinical Trial.
-
Endovascular treatment for large-core ischaemic stroke: a meta-analysis of randomised controlled clinical trials.J Neurol Neurosurg Psychiatry. 2023 Oct;94(10):781-785. doi: 10.1136/jnnp-2023-331513. Epub 2023 Jul 14. J Neurol Neurosurg Psychiatry. 2023. PMID: 37451694
-
Endovascular thrombectomy vs best medical management for late presentation acute ischaemic stroke with large vessel occlusion without CT perfusion or MR imaging selection: A systematic review and meta-analysis.J Stroke Cerebrovasc Dis. 2024 Nov;33(11):108002. doi: 10.1016/j.jstrokecerebrovasdis.2024.108002. Epub 2024 Sep 7. J Stroke Cerebrovasc Dis. 2024. PMID: 39245396
References
-
- Berkhemer OA, Fransen PS, Beumer D. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 2015; 372: 394–420. - PubMed
-
- Goyal M, Menon BK, van Zwam WH, et al.. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet 2016; 387: 1723–1731. - PubMed
LinkOut - more resources
Full Text Sources
