

Cardiopulmonary exercise testing parameters in healthy athletes vs. equally fit individuals with hypertrophic cardiomyopathy
- PMID: 40320900
- PMCID: PMC12212187
- DOI: 10.1093/eurjpc/zwaf177
Cardiopulmonary exercise testing parameters in healthy athletes vs. equally fit individuals with hypertrophic cardiomyopathy
Abstract
Aims: Cardiopulmonary exercise testing (CPET) is often used when athletes present with suspected hypertrophic cardiomyopathy (HCM). While low peak oxygen consumption (pV˙O2) augments concern for HCM, athletes with HCM frequently display supranormal pV˙O2, which limits this parameter's diagnostic utility. We aimed to compare other CPET parameters in healthy athletes and equally fit individuals with HCM.
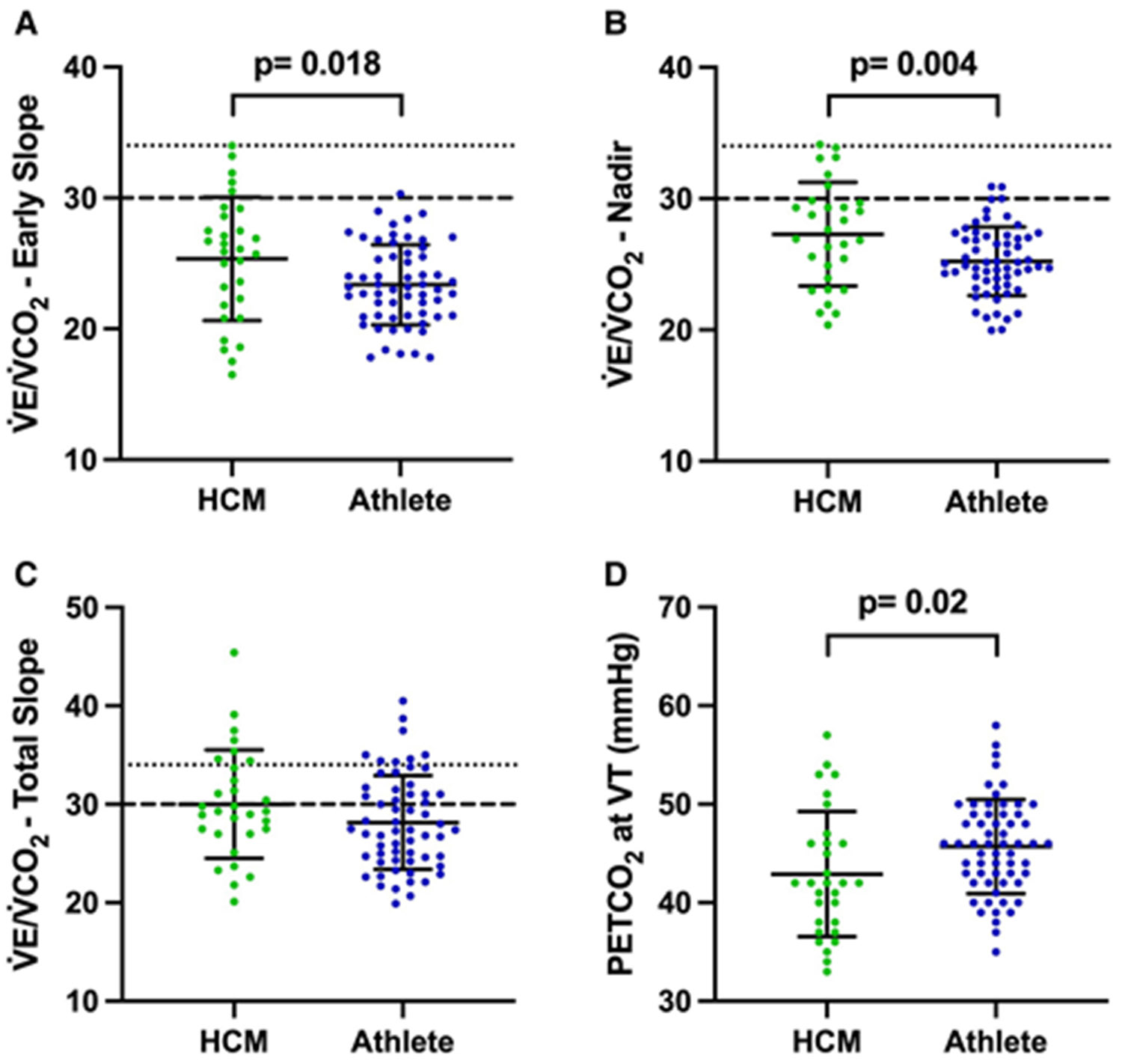
Methods and results: Using cycle ergometer CPETs from a single centre, we compared ventilatory efficiency and recovery kinetics between individuals with HCM [percent predicted pV˙O2(ppV˙O2) > 80%, non-obstructive, no nodal agents] and healthy athletes, matched (2:1 ratio) for age, sex, height, weight and ppV˙O2. Consistent with matching, HCM (n = 30, 43.6 ± 14.2 years) and athlete (n = 60, 43.8 ± 14.9 years) groups had similar, supranormal pV˙O2 (39.5 ± 9.1 vs. 41.1 ± 9.1 mL/kg/min, 125 ± 26 vs. 124 ± 25% predicted). Recovery kinetics were also similar. However, HCM participants had worse ventilatory efficiency, including higher early V˙E/V˙CO2 slope (25.4 ± 4.7 vs. 23.4 ± 3.1, P = 0.02), higher V˙E/V˙CO2 nadir (27.3 ± 4.0 vs. 25.2 ± 2.6, P = 0.004) and lower end-tidal CO2 at the ventilatory threshold (42.9 ± 6.4 vs. 45.7 ± 4.8 mmHg, P = 0.02). HCM participants were more likely to have abnormally high V˙E/V˙CO2 nadir (>30) than athletes (20 vs. 3%, P = 0.02).
Conclusion: Even in the setting of similar and supranormal pV˙O2, ventilatory efficiency is worse in HCM participants vs. healthy athletes. Our results demonstrate the utility of CPET beyond pV˙O2 assessment in 'grey zone' athlete cases in which the diagnosis of HCM is being debated.
Keywords: Athlete’s heart; Cardiopulmonary exercise testing; Hypertrophic cardiomyopathy.
Plain language summary
We sought to examine exercise test findings in healthy athletes and equally fit individuals with a form of heart enlargement that commonly gets confused with ‘athlete’s heart’ called hypertrophic cardiomyopathy (HCM) to see if elements of the exercise test could distinguish between these two groups. This is relevant as fit individuals often present for exercise testing as part of the work up to see if they have HCM or not, and getting the answer right is important because HCM is amongst the most common causes of sudden cardiac death in athletes.By design, individuals with HCM in this study were equally fit as the athletes, with both groups having fitness levels (‘VO2 max’ levels) around 25% higher than expected for individuals of similar age and sex.Despite this similar and supranormal fitness, individuals with HCM had worse ventilatory efficiency than athletes. This is a metric that reflects how well the heart and lungs work together to get rid of the waste gas carbon dioxide during exercise. This finding should focus more attention on this parameter when exercise tests are being performed to evaluate for HCM in clinical practice.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: none declared.
Figures
Comment in
-
Exercise ventilation inefficiency in fit subjects with hypertrophic cardiomyopathy: a new 'red flag' in the diagnostic process of the negative cardiac phenotype?Eur J Prev Cardiol. 2025 Sep 8;32(12):1120-1121. doi: 10.1093/eurjpc/zwaf255. Eur J Prev Cardiol. 2025. PMID: 40264214 No abstract available.
References
-
- Sheikh N, Papadakis M, Schnell F, Panoulas V, Malhotra A, Wilson M, et al. Clinical profile of athletes with hypertrophic cardiomyopathy. Circ Cardiovasc Imaging 2015;8:e003454. - PubMed
-
- Martinez MW, Kim JH, Shah AB, Phelan D, Emery MS, Wasfy MM, et al. Exercise-induced cardiovascular adaptations and approach to exercise and cardiovascular disease: JACC state-of-the-art review. J Am Coll Cardiol 2021;78:1453–1470. - PubMed
-
- Sharma S, Elliott P, Whyte G, Jones S, Mahon N, Whipp B, et al. Utility of cardiopulmonary exercise in the assessment of clinical determinants of functional capacity in hypertrophic cardiomyopathy. Am J Cardiol 2000;86:162–168. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
