

Stress hyperglycemia ratio as a predictor of acute kidney injury and its outcomes in critically ill patients
- PMID: 40321025
- PMCID: PMC12054585
- DOI: 10.1080/0886022X.2025.2499228
Stress hyperglycemia ratio as a predictor of acute kidney injury and its outcomes in critically ill patients
Abstract
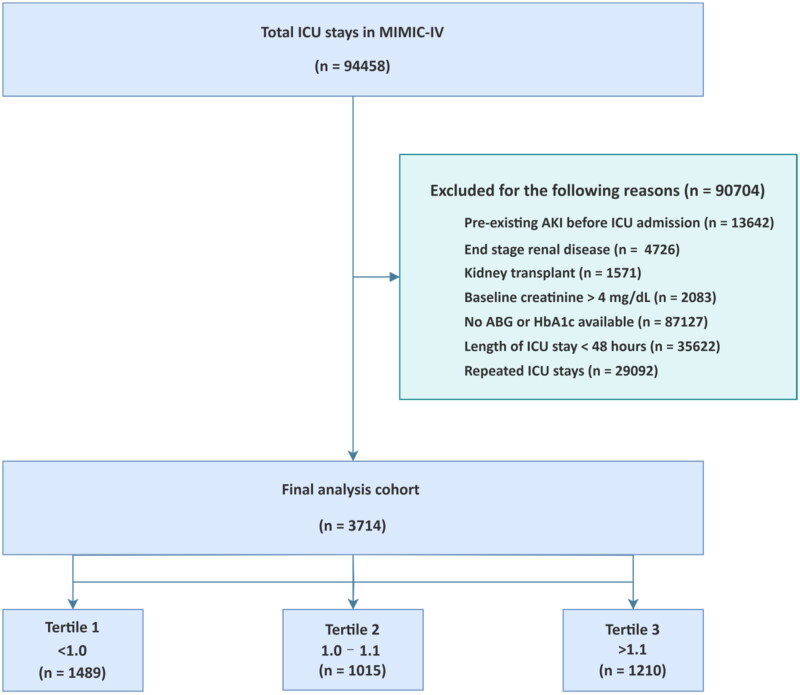
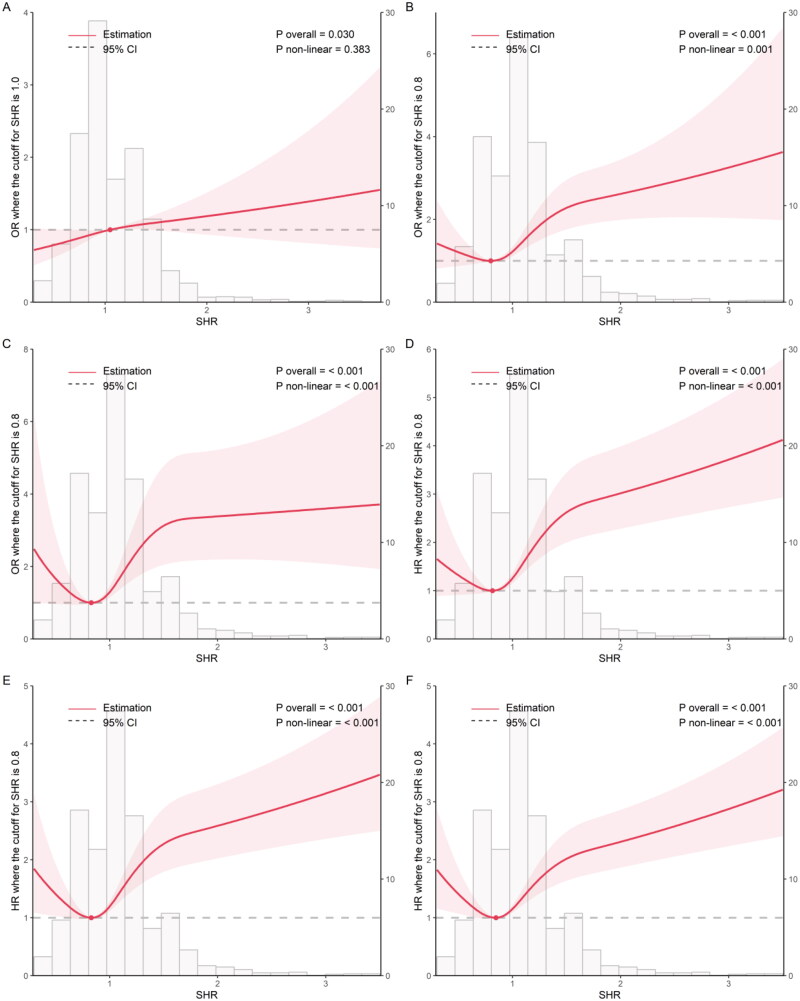
This study investigated stress hyperglycemia ratio (SHR) for acute kidney injury (AKI) and clinical outcomes in intensive care unit (ICU). Key outcomes were AKI within 48 h after ICU admission, acute kidney disease (AKD), ICU mortality, 28-day mortality, 90-day mortality and 1-year mortality. The associations between SHR and outcomes was estimated via logistic regression, Cox proportional hazards regression, and restricted cubic spline (RCS) analyses. Subgroup analyses assessed the consistency of these associations. Totally 3,714 patients were included from the Medical Information Mart for Intensive Care IV. SHR was associated with an increased risk of AKI (ORadjusted 1.29 95%CI 1.05-1.59). Among AKI patients, SHR was associated with increased risks of AKD (ORadjusted 1.94 95%CI 1.57-2.39), ICU mortality (ORadjusted 2.31 95%CI 1.60-3.32), 28-day mortality (HRadjusted 1.39 95%CI 1.29-1.50), 90-day mortality (HRadjusted 1.37 95%CI 1.26-1.48), and 1-year mortality (HRadjusted 1.37 95%CI 1.27-1.47). RCS analysis revealed a linear relationship with AKI, a J-shaped relationship with AKD, and a U-shaped relationship with mortality. Subgroup analysis confirmed the consistency of relationship between SHR and AKI. SHR demonstrates significant associations with AKI incidence, and correlates with AKD progression/mortality in critically ill adult ICU patients, suggesting its potential as a risk stratification and prognostic tool for AKI management, though further prospective validation is required.
Keywords: Stress hyperglycemia ratio; acute kidney disease; acute kidney injury; intensive care unit; mortality.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as being potential conflicts of interest.
Figures
Similar articles
-
Stress hyperglycemia ratio as an independent predictor of acute kidney injury in critically ill patients with acute myocardial infarction: a retrospective U.S. cohort study.Ren Fail. 2025 Dec;47(1):2471018. doi: 10.1080/0886022X.2025.2471018. Epub 2025 Feb 26. Ren Fail. 2025. PMID: 40012169 Free PMC article.
-
The association between acute kidney injury and dysglycaemia in critically ill patients with and without diabetes mellitus: a retrospective single-center study.Ren Fail. 2024 Dec;46(2):2397555. doi: 10.1080/0886022X.2024.2397555. Epub 2024 Sep 4. Ren Fail. 2024. PMID: 39230066 Free PMC article.
-
Association between stress hyperglycemia ratio (SHR) and the risk of acute kidney injury in patients with chronic kidney disease: analysis of the MIMIC-IV database.BMC Nephrol. 2025 Jul 1;26(1):310. doi: 10.1186/s12882-025-04212-1. BMC Nephrol. 2025. PMID: 40597740 Free PMC article.
-
Association between stress hyperglycemia ratio and acute kidney injury development in patients with sepsis: a retrospective study.Front Endocrinol (Lausanne). 2025 Apr 15;16:1542591. doi: 10.3389/fendo.2025.1542591. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40303646 Free PMC article.
-
Blood Pressure and the Risk of Acute Kidney Injury in the ICU: Case-Control Versus Case-Crossover Designs.2016 Sep 10. In: MIT Critical Data, editor. Secondary Analysis of Electronic Health Records [Internet]. Cham (CH): Springer; 2016. Chapter 25. 2016 Sep 10. In: MIT Critical Data, editor. Secondary Analysis of Electronic Health Records [Internet]. Cham (CH): Springer; 2016. Chapter 25. PMID: 31314276 Free Books & Documents. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical