

Acute Valve Syndrome in Aortic Stenosis
- PMID: 40321310
- PMCID: PMC12047511
- DOI: 10.1016/j.shj.2024.100377
Acute Valve Syndrome in Aortic Stenosis
Abstract
Background: To describe the impact of clinical presentation among patients with aortic stenosis (AS) undergoing aortic valve replacement (AVR).
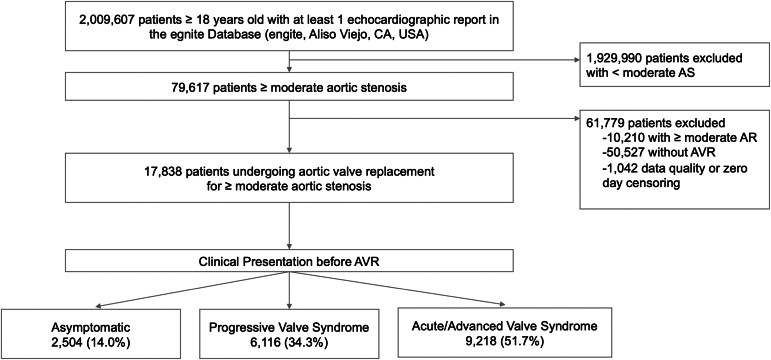
Methods: We analyzed a real-world dataset including patients from 29 US hospitals (egnite Database, egnite). Patients over 18 years old with moderate or greater AS undergoing AVR were included. Patients were classified into 3 groups according to the acuity and severity of clinical presentation prior to AVR: (i) asymptomatic, (ii) progressive signs and symptoms (progressive valve syndrome [PVS]), and (iii) acute or advanced signs and symptoms (acute valve syndrome [AVS]). Mortality and heart failure hospitalization after AVR were examined with Kaplan-Meier estimates, with results compared using the log-rank test.
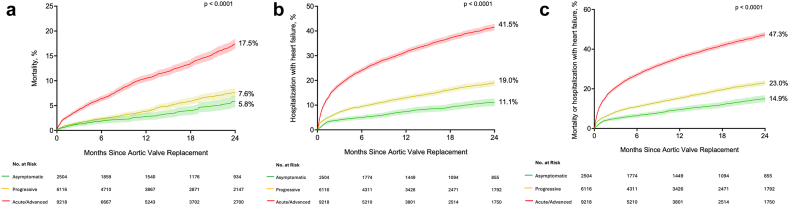
Results: Among 2,009,607 patients in our database, 17,838 underwent AVR (78.6% transcatheter AVR, 21.4% surgical AVR). Age was 76.5 ± 9.7 years, and 40.2% were female. Prior to AVR, 2504 (14.0%) were asymptomatic, 6116 (34.3%) presented with PVS, and 9218 (51.7%) presented with AVS. At 2 years, the estimated rate of mortality for asymptomatic, PVS, and AVS were 5.8% (4.6%-7.0%), 7.6% (6.7%-8.4%), and 17.5% (16.5%-18.5%), respectively, and the estimated rate of hospitalization with heart failure for asymptomatic, PVS, and AVS were 11.1% (9.5%-12.6%), 19.0% (17.8%-20.2%), and 41.5% (40.2%-42.8%), respectively. After adjustment, patients presenting with AVS had increased risk of mortality after AVR (hazard ratio, 2.2; 95% CI, 1.8-2.6).
Conclusions: From a large, real-world database of patients undergoing AVR for AS, most patients presented with AVS, which was associated with an increased risk of mortality and heart failure hospitalization.
Keywords: Aortic stenosis; Aortic valve; Aortic valve replacement; Clinical presentation; Transcatheter aortic valve implantation; Transcatheter aortic valve replacement.
© 2024 The Author(s).
Figures


Similar articles
-
The Mortality Burden of Untreated Aortic Stenosis.J Am Coll Cardiol. 2023 Nov 28;82(22):2101-2109. doi: 10.1016/j.jacc.2023.09.796. Epub 2023 Oct 24. J Am Coll Cardiol. 2023. PMID: 37877909
-
Rehospitalization Events After Aortic Valve Replacement: Insights From the PARTNER Trial.Circ Cardiovasc Interv. 2022 Dec;15(12):e012195. doi: 10.1161/CIRCINTERVENTIONS.122.012195. Epub 2022 Dec 20. Circ Cardiovasc Interv. 2022. PMID: 36538580 Clinical Trial.
-
Prognostic significance of LGE by CMR in aortic stenosis patients undergoing valve replacement.J Am Coll Cardiol. 2014 Jul 15;64(2):144-54. doi: 10.1016/j.jacc.2014.02.612. J Am Coll Cardiol. 2014. PMID: 25011718
-
Renin-Angiotensin System Blockade in Aortic Stenosis: Implications Before and After Aortic Valve Replacement.J Am Heart Assoc. 2020 Sep 15;9(18):e016911. doi: 10.1161/JAHA.120.016911. Epub 2020 Sep 6. J Am Heart Assoc. 2020. PMID: 32893727 Free PMC article. Review.
-
Optimal Threshold of Left Ventricular Ejection Fraction for Aortic Valve Replacement in Asymptomatic Severe Aortic Stenosis: A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2021 Apr 6;10(7):e020252. doi: 10.1161/JAHA.120.020252. Epub 2021 Mar 31. J Am Heart Assoc. 2021. PMID: 33787311 Free PMC article.
References
-
- Landes U., Orvin K., Codner P., et al. Urgent transcatheter aortic valve implantation in patients with severe aortic stenosis and acute heart failure: procedural and 30-day outcomes. Can J Cardiol. 2016;32:726–731. - PubMed
-
- Kolte D., Khera S., Vemulapalli S., et al. Outcomes following urgent/emergent transcatheter aortic valve replacement: insights from the STS/ACC TVT Registry. JACC Cardiovasc Interv. 2018;11:1175–1185. - PubMed
-
- Wald D.S., Williams S., Bangash F., Bestwick J.P. Watchful waiting in aortic stenosis: the problem of acute decompensation. Am J Med. 2018;131:173–177. - PubMed
-
- Kaewkes D., Ochiai T., Flint N., et al. Transcatheter aortic valve implantation in patients with severe aortic stenosis hospitalized with acute heart failure. Am J Cardiol. 2021;144:100–110. - PubMed
-
- Popovic B., Molho A., Varlot J., et al. Prognostic influence of acute decompensated heart failure in patients planned for transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2020;96:E542–E551. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
