

Challenging the Dogma of Dead Space Obliteration With Muscle Flaps in Deep Spinal Surgical Site Infections
- PMID: 40321322
- PMCID: PMC12045538
- DOI: 10.1097/GOX.0000000000006732
Challenging the Dogma of Dead Space Obliteration With Muscle Flaps in Deep Spinal Surgical Site Infections
Abstract
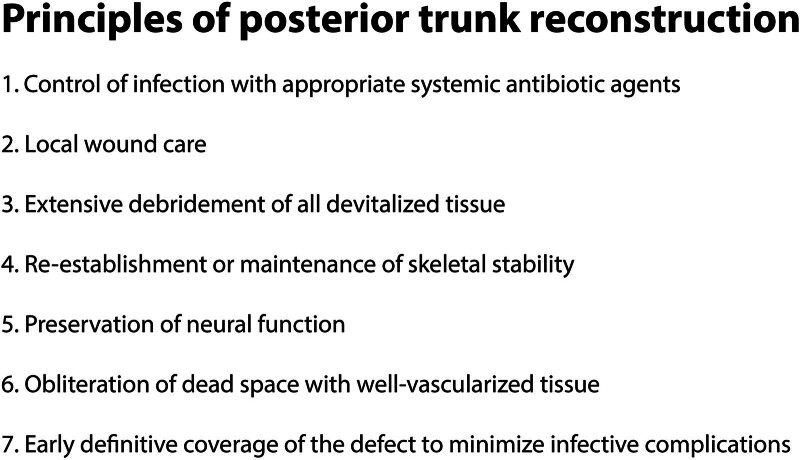
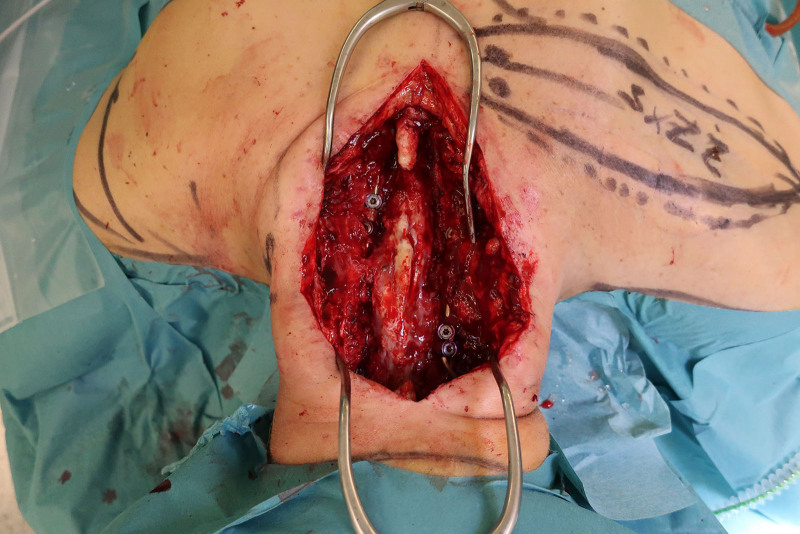
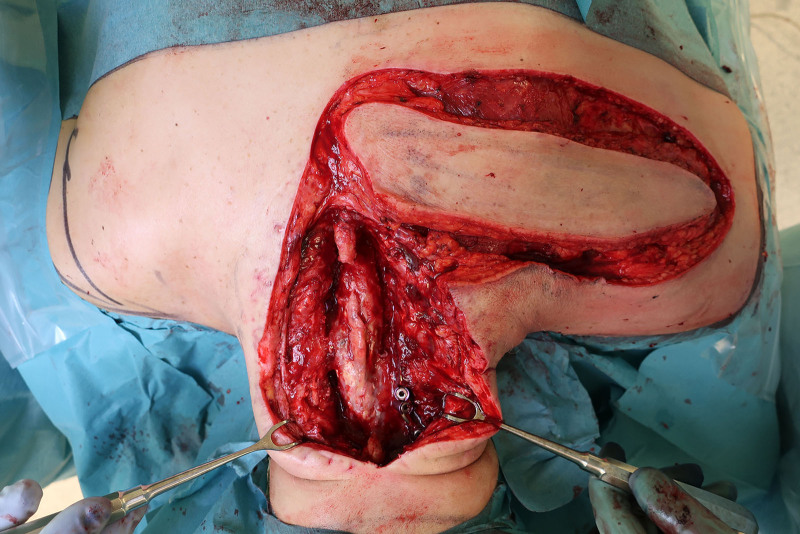
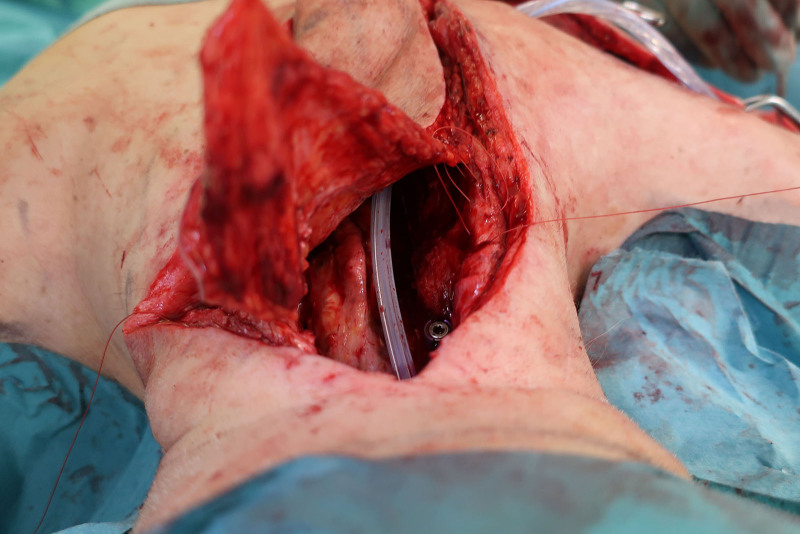
Background: A deep surgical site infection (SSI) after spinal surgery is a serious complication. The defect formed is often a complex 3-dimensional dead space due to tissue loss, frequently containing spinal hardware. Traditionally, obliteration of that dead space is performed with the use of muscle flaps. We challenge this dogma in reconstructive surgery by using the medial dorsal intercostal artery perforator (MDICAP) flap as an alternative in the reconstruction. It adheres to the concept of replacing "like with like," as there are no muscles at the posterior midline.
Methods: A retrospective study was performed of a cohort of 18 patients with deep SSI and a posterior midline defect after spinal surgery who received reconstruction with the MDICAP flap. A review of postoperative imaging with focus on dead space was performed.
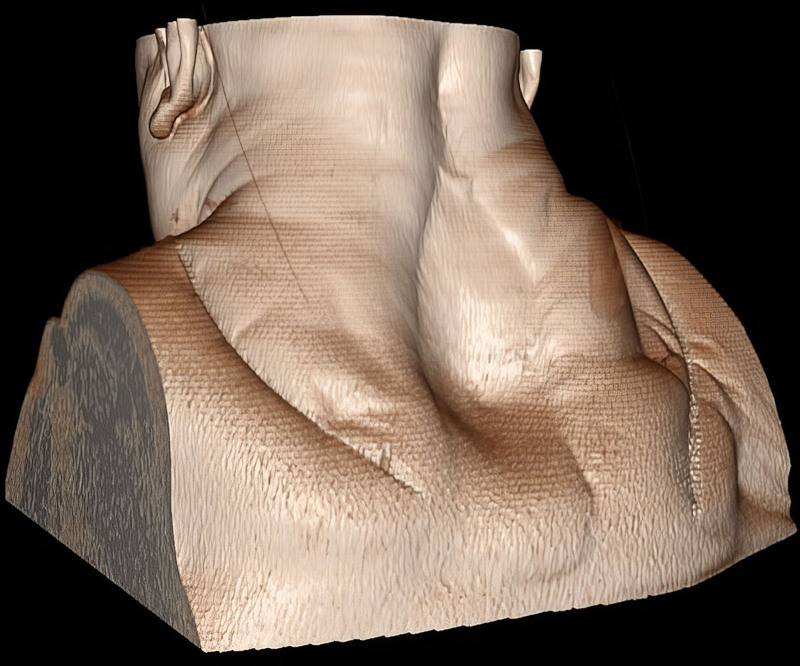
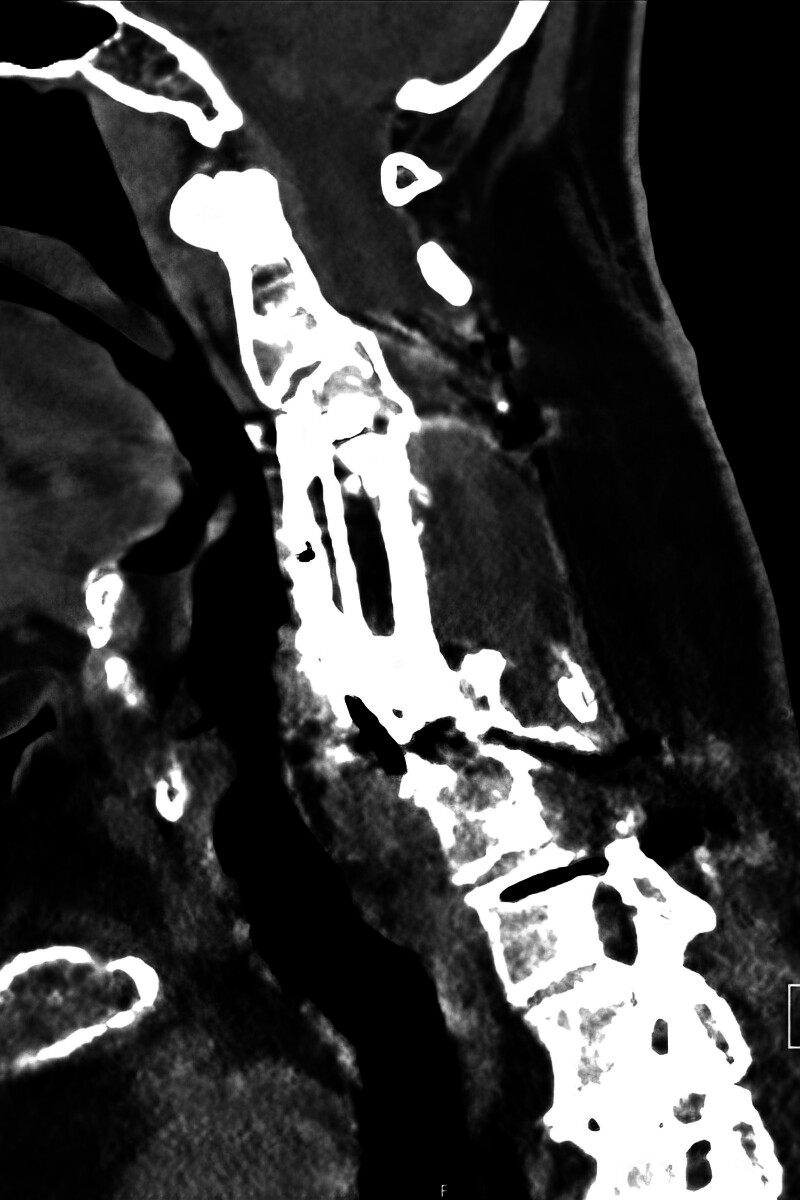
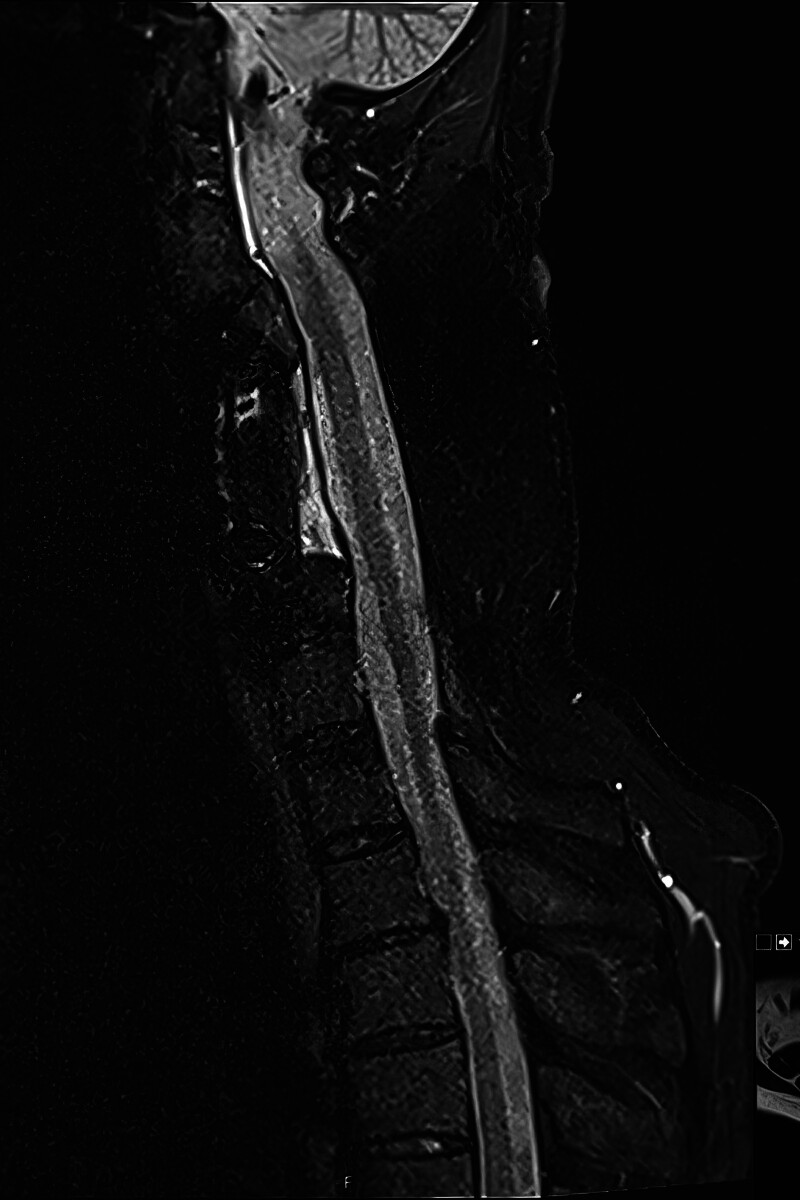
Results: All patients had satisfactory functional and aesthetic outcomes. No patients had a recurrent deep SSI during follow-up (average 64 mo, range 3-384 mo). In the 16 patients who had postoperative imaging performed, dead space was not present at the flaps' recipient site.
Conclusions: The MDICAP flap is a good alternative to muscle flaps in reconstructive surgery for complex posterior midline defects caused by a deep SSI after spinal surgery. Postoperative imaging showed no dead space with the use of MDICAP flaps. All patients had an uneventful postoperative course with no recurrent infections. This challenges the dogmata of (1) the need for muscle flaps in such reconstruction and (2) the obligate need for dead space obliteration at the time of operation.
Copyright © 2025 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
The authors have no financial interest to declare in relation to the content of this article.
Figures




Similar articles
-
Closure of Complex Posterior Midline Defects After Spinal Surgery With Sensate Midline-based Perforator Flaps and the Long-term Results.Spine (Phila Pa 1976). 2015 Dec;40(23):E1233-8. doi: 10.1097/BRS.0000000000001048. Spine (Phila Pa 1976). 2015. PMID: 26165215
-
Reconstruction of soft tissue defect around knee with thoracodorsal artery perforator flap and muscle-sparing latissimus dorsi flap.Microsurgery. 2023 Oct;43(7):665-675. doi: 10.1002/micr.31024. Epub 2023 Feb 15. Microsurgery. 2023. PMID: 36789684
-
Lumbar Perforator Flaps for Coverage of Extensive Defects With Osteomyelitis.Ann Plast Surg. 2021 Jan;86(1):67-71. doi: 10.1097/SAP.0000000000002399. Ann Plast Surg. 2021. PMID: 33306501
-
Combined use of lower medial thigh perforator (LMTP) flap and pedicled medial sural artery perforator flap (MSAP) for lateral knee defects coverage after sarcoma resection: A case report and literature review of soft tissue defect around knee reconstruction.Microsurgery. 2024 Jan;44(1):e31125. doi: 10.1002/micr.31125. Epub 2023 Oct 13. Microsurgery. 2024. PMID: 37830398 Review.
-
One-stage reconstruction of composite bone and soft-tissue defects in traumatic lower extremities.Plast Reconstr Surg. 2004 Nov;114(6):1457-66. doi: 10.1097/01.prs.0000138811.88807.65. Plast Reconstr Surg. 2004. PMID: 15509933 Review.
References
-
- Halsted WS. The treatment of wounds with especial reference to the value of the blood clot in the management of dead spaces. Johns Hopkins Hosp Rep. 1890;2:255–314.
-
- Neuber G. Vorschläge zur Beseitigung der Drainage für alle frischen Wunden. DMW Dtsch Med Wochenschr. 1884;10:458–458.
-
- Küster E. Über die Anwendung versenkter Nähte insbesondere bei plastischen Operationen. Verh Dtsch Ges Chir. 1884;13:62.
-
- Rohrich RJ, Timberlake AT, Afrooz PN. Revisiting the fundamental operative principles of plastic surgery. Plast Reconstr Surg. 2021;148:117S–120S. - PubMed
-
- Freire-Archer M, Sarraj M, Koziarz A, et al. . Incidence and recurrence of deep spine surgical site infections: a systematic review and meta-analysis. Spine (Phila Pa 1976). 2023;48:E269–E285. - PubMed
LinkOut - more resources
Full Text Sources