

Establishment and validation of a nomogram for predicting IDH-wildtype glioblastomas in nonenhancing adult-type diffuse gliomas
- PMID: 40321617
- PMCID: PMC12048881
- DOI: 10.1093/noajnl/vdaf035
Establishment and validation of a nomogram for predicting IDH-wildtype glioblastomas in nonenhancing adult-type diffuse gliomas
Abstract
Background: Approximately 8.94%-44.44% of nonenhancing adult-type diffuse gliomas are identified as glioblastomas. Our purpose is to develop a nomogram that can predict glioblastomas from nonenhancing adult-type diffuse gliomas.
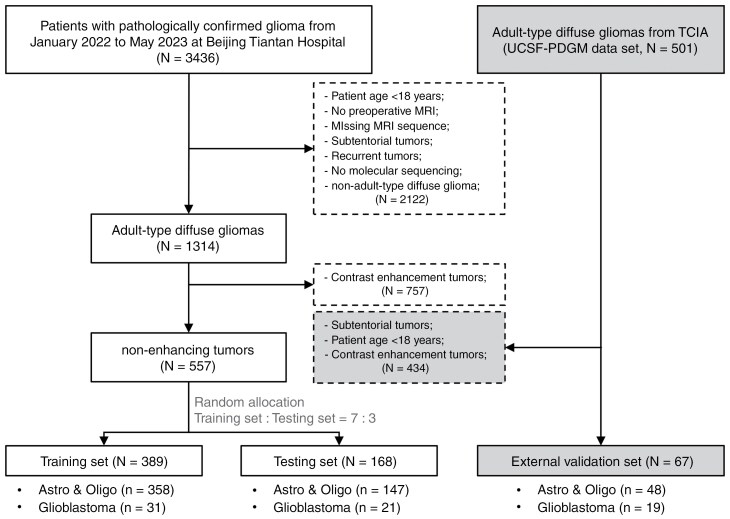
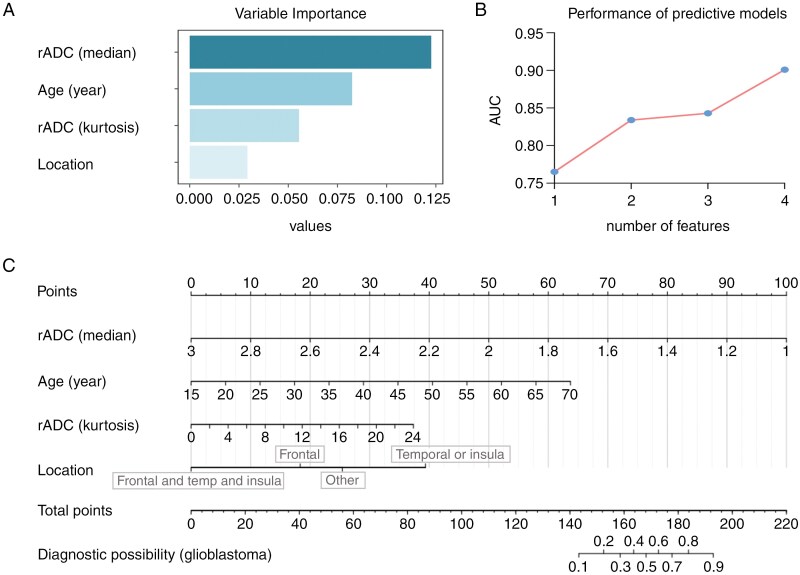
Methods: Nonenhancing adult-type diffuse gliomas were collected from Beijing Tiantan Hospital and TCIA public database. Univariate and multivariate logistic regression were performed to screen features on the training set. The features with P < .05 in multivariate logistic regression were used to establish the prediction model. The testing and validation sets were used to test the model.
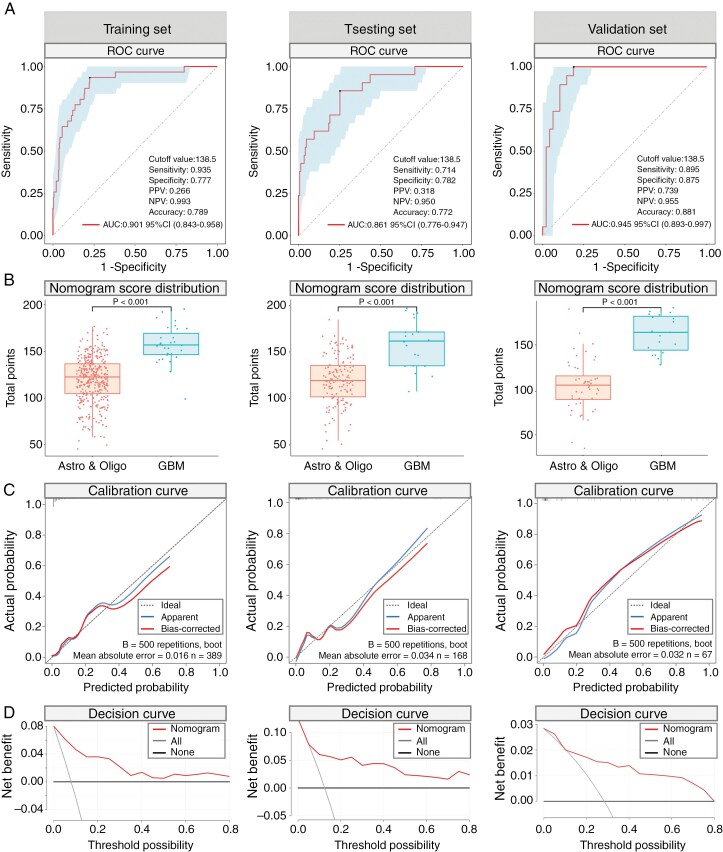
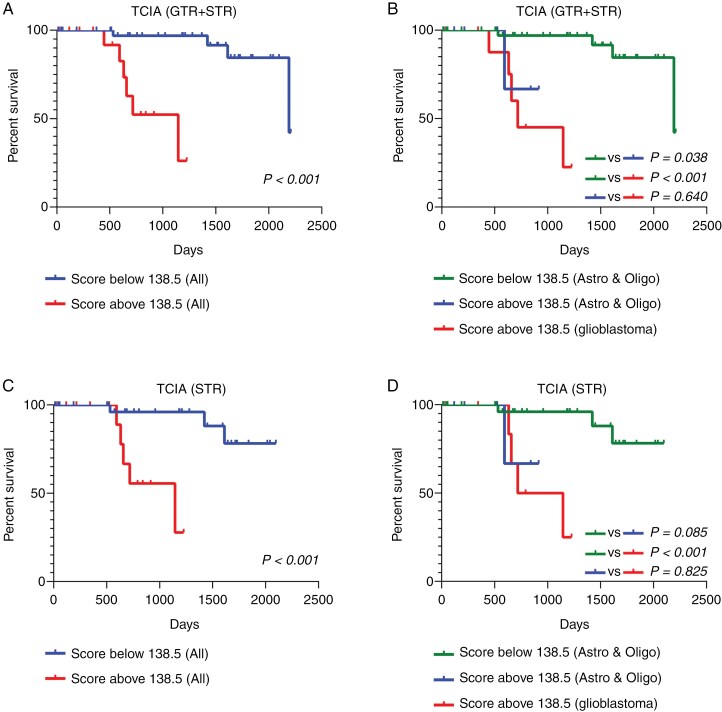
Results: A total of 557 and 67 nonenhancing adult-type diffuse gliomas were collected from Beijing Tiantan Hospital and TCIA, respectively. The T2-FLAIR mismatch sign exhibited 100% specificity but low sensitivity (<30%) in ruling out glioblastoma. Age, tumor location, rADC(kurtosis), and rADC(median) were identified as independent predictors and employed for developing the prediction model. The AUC of the model was 0.901, 0.861, and 0.945 in the training, testing, and validation set, respectively. The best cutoff value of nomoscore was 138.5, which achieved sensitivity of 0.935, 0.714, and 0.895, specificity of 0.777, 0.782, and 0.8775 in the training, testing, and validation sets, respectively. Survival analysis shown that patients with nomoscore above 138.5 had significantly poorer survival time than those with scores below 138.5.
Conclusions: Positive T2-FLAIR mismatch sign can effectively rule out glioblastoma in nonenhancing adult-type diffuse gliomas with high specificity. Nonenhancing adult-type diffuse gliomas with nomoscore above 138.5 are highly suspicious for glioblastoma or nonglioblastoma with a poor prognosis.
Keywords: adult-type diffuse glioma; glioblastoma; nomogram; nonenhancing; prognosis.
© The Author(s) 2025. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Figures
Similar articles
-
Identifying IDH-mutant and 1p/19q noncodeleted astrocytomas from nonenhancing gliomas: Manual recognition followed by artificial intelligence recognition.Neurooncol Adv. 2024 Feb 1;6(1):vdae013. doi: 10.1093/noajnl/vdae013. eCollection 2024 Jan-Dec. Neurooncol Adv. 2024. PMID: 38405203 Free PMC article.
-
Advanced imaging parameters improve the prediction of diffuse lower-grade gliomas subtype, IDH mutant with no 1p19q codeletion: added value to the T2/FLAIR mismatch sign.Eur Radiol. 2020 Feb;30(2):844-854. doi: 10.1007/s00330-019-06395-2. Epub 2019 Aug 24. Eur Radiol. 2020. PMID: 31446467
-
MRI Scoring Systems for Predicting Isocitrate Dehydrogenase Mutation and Chromosome 1p/19q Codeletion in Adult-type Diffuse Glioma Lacking Contrast Enhancement.Radiology. 2024 May;311(2):e233120. doi: 10.1148/radiol.233120. Radiology. 2024. PMID: 38713025
-
The T2-FLAIR-mismatch sign as an imaging biomarker for IDH and 1p/19q status in diffuse low-grade gliomas: a systematic review with a Bayesian approach to evaluation of diagnostic test performance.Neurosurg Focus. 2019 Dec 1;47(6):E13. doi: 10.3171/2019.9.FOCUS19660. Neurosurg Focus. 2019. PMID: 31786548
-
Advanced Magnetic Resonance Imaging in Pediatric Glioblastomas.Front Neurol. 2021 Nov 10;12:733323. doi: 10.3389/fneur.2021.733323. eCollection 2021. Front Neurol. 2021. PMID: 34858308 Free PMC article. Review.
References
-
- Park YW, Kim S, Han K, et al.Rethinking extent of resection of contrast-enhancing and non-enhancing tumor: different survival impacts on adult-type diffuse gliomas in 2021 World Health Organization classification. Eur Radiol. 2024;34(2):1376–1387. - PubMed
LinkOut - more resources
Full Text Sources