

Nephrologist's Perceptions of Risk of Severe Chronic Kidney Disease and Outpatient Follow-up After Hospitalization With AKI: Multinational Randomized Survey Study
- PMID: 40321680
- PMCID: PMC12046161
- DOI: 10.1177/20543581251336548
Nephrologist's Perceptions of Risk of Severe Chronic Kidney Disease and Outpatient Follow-up After Hospitalization With AKI: Multinational Randomized Survey Study
Abstract
Background: Patients hospitalized with acute kidney injury (AKI) have variable risks for chronic kidney disease (CKD); however, there is limited knowledge about how this risk influences outpatient follow-up with nephrologists.
Objective: This survey study examined the likelihood that nephrologists would recommend outpatient follow-up of patients with varying risk profiles for CKD after hospitalization with AKI and the effect of reporting the predicted risk of severe CKD on their decision-making.
Design: A randomized survey study examining the impact of providing predicted risks of severe CKD on nephrologists' follow-up recommendations for patients with AKI.
Setting: The study included nephrologists from the United States, the United Kingdom, and Canada between September and December 2023.
Patients: Participants reviewed clinical vignettes of patients with AKI and varying risks of severe CKD (G4 or G5), using an externally validated prediction model.
Measurements: The primary outcome was the likelihood of recommending nephrologist specialist follow-up for each case, scored on a 7-point Likert scale (1 = "definitely not" and 7 = "definitely would").
Methods: Participants were randomized to receive a version of the survey either with or without the predicted risk of severe CKD included for each vignette. Responses were compared across categories of predicted risk (<10%, 10%-49%, and ≥50%) using generalized estimating equations.
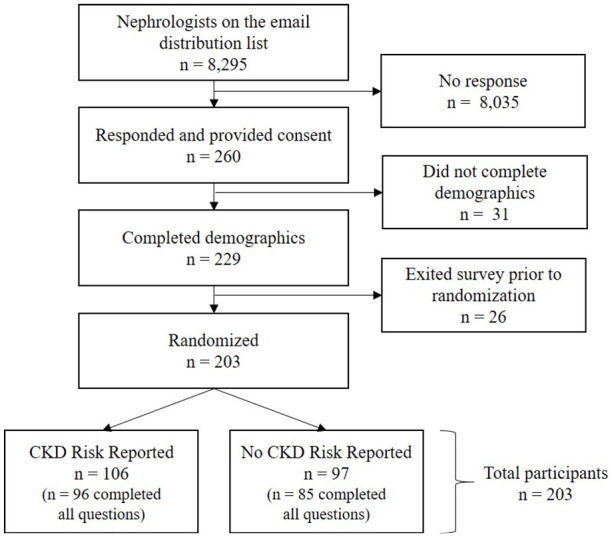
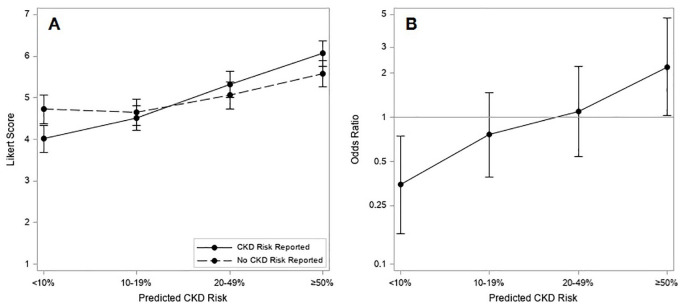
Results: Of the 203 nephrologists who participated, 73 (36%) were from the United Kingdom, 71 (35%) from Canada, and 45 (22%) from the United States. Mean (95% confidence interval [CI]) Likert scores increased from 4.01 (3.68, 4.34) for patients with a <10% predicted risk to 6.06 (5.76, 6.37) for those with a ≥ 50% predicted risk of severe CKD. Nephrologists were significantly less likely to recommend outpatient nephrology follow-up for patients with a <10% predicted risk of severe CKD when the risk was reported (mean difference = -0.71 [95% CI = -1.19, -0.23]), and significantly more likely to recommend follow-up for patients with a ≥50% predicted risk when the risk of severe CKD was reported (mean difference = 0.49 [95% CI = 0.04, 0.93]).
Limitations: This study focuses on nephrologists from high-income countries and relies on hypothetical scenarios rather than real-world practices. Survey respondents may not be representative of all nephrologists, although consistent findings across diverse subgroups strengthen findings.
Conclusions: When the predicted risk of severe CKD is reported, nephrologists are less likely to recommend follow-up for lower risk patients with AKI and more likely to recommend follow-up for higher risk patients, leading to better alignment of recommendations for outpatient follow-up with patient risk of severe CKD.
Contexte: Les patients hospitalisés pour insuffisance rénale aiguë (IRA) présentent un risque variable d’évoluer vers l’insuffisance rénale chronique (IRC). On ignore toutefois si ce risque influence la décision des néphrologues de recommander un suivi en ambulatoire.
Objectif: Étude par sondage examinant la probabilité que les néphrologues recommandent un suivi en ambulatoire à des patients hospitalisés pour IRA et présentant divers profils de risque d’évoluer vers l’IRC. On souhaitait également vérifier si la mention du risque prévu d’IRC grave influençait la prise de décision.
Conception: Étude randomisée examinant l’impact de la divulgation du risque prévu d’IRC grave des patients hospitalisés pour IRA sur la possibilité qu’ils soient aiguillés pour un suivi en ambulatoire par un néphrologue.
Cadre: Sondage auprès de néphrologues des États-Unis, du Royaume-Uni et du Canada entre septembre et décembre 2023.
Sujets: À l’aide d’un modèle prédictif validé en externe, les néphrologues participants ont examiné les cas cliniques de patients hospitalisés pour IRA et présentant des risques variables d’évoluer vers l’IRC grave (G4 ou G5).
Mesures: Pour chaque cas, le principal critère d’évaluation était la probabilité de recommander un suivi spécialisé par un néphrologue, évaluée à l’aide d’une échelle de Likert à sept points (1 = « certainement pas », 7 = « très certainement »).
Méthodologie: Les néphrologues participants ont été répartis aléatoirement pour recevoir une version du sondage avec ou sans mention du risque prévu d’IRC grave pour chaque cas clinique. Les réponses ont été comparées selon la catégorie de risque prévu (<10 %, 10 à 49 % et ≥50 %) à l’aide d’équations d’estimation généralisées.
Résultats: Des 203 néphrologues participants, 73 (36 %) provenaient du Royaume-Uni, 71 (35 %) du Canada et 45 (22 %) des États-Unis. Les scores de Likert moyens sont passés de 4,01 (IC95: 3,68 à 4,34), pour les cas où le risque prévu d’IRC grave était inférieur à 10 %, à 6,06 (IC95: 5,76 à 6,37) pour les cas où ce risque était égal ou supérieur à 50 %. Lorsque le risque prévu d’IRC grave était indiqué, les néphrologues étaient significativement moins enclins à recommander un suivi en ambulatoire aux patients présentant un risque prévu inférieur à 10 % (diff. moy.: -0,71 [IC95: -1,19 à - 0,23]) et plus enclins à le faire si ce risque était d’au moins 50 % (diff. moy.: 0,49 [IC95: 0,04 à 0,93]).
Limites: L’étude repose sur des scénarios hypothétiques plutôt que sur des pratiques réelles. Seuls des néphrologues provenant de pays à revenu élevé ont été interrogés; ces derniers pourraient ne pas être représentatifs de l’ensemble des néphrologues, bien que des résultats comparables obtenus dans divers sous-groupes renforcent les résultats de la présente étude.
Conclusion: Dans les cas où le risque prévu d’évolution vers l’IRC grave est indiqué, les néphrologues sont moins enclins à recommander un suivi aux patients hospitalisés pour IRA dont le risque prévu d’IRC grave est faible, et plus enclins à le faire pour les patients dont le risque prévu est élevé. Ceci permet une plus grande cohérence dans les recommandations de suivi ambulatoire pour les patients présentant un risque d’évoluer vers l’IRC grave.
Keywords: acute kidney disease; chronic kidney disease; kidney health; nephrologist follow-up; risk stratification.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Neyra JA, Silver SA. We won’t get fooled again: finding the who to follow after acute kidney injury. Am J Kidney Dis. 2021;78(1):16-18. - PubMed
LinkOut - more resources
Full Text Sources
