

Simple electrocardiographic index for A4-wave amplitude of the VDD leadless pacemaker
- PMID: 40321726
- PMCID: PMC12047474
- DOI: 10.1016/j.hroo.2025.01.006
Simple electrocardiographic index for A4-wave amplitude of the VDD leadless pacemaker
Abstract
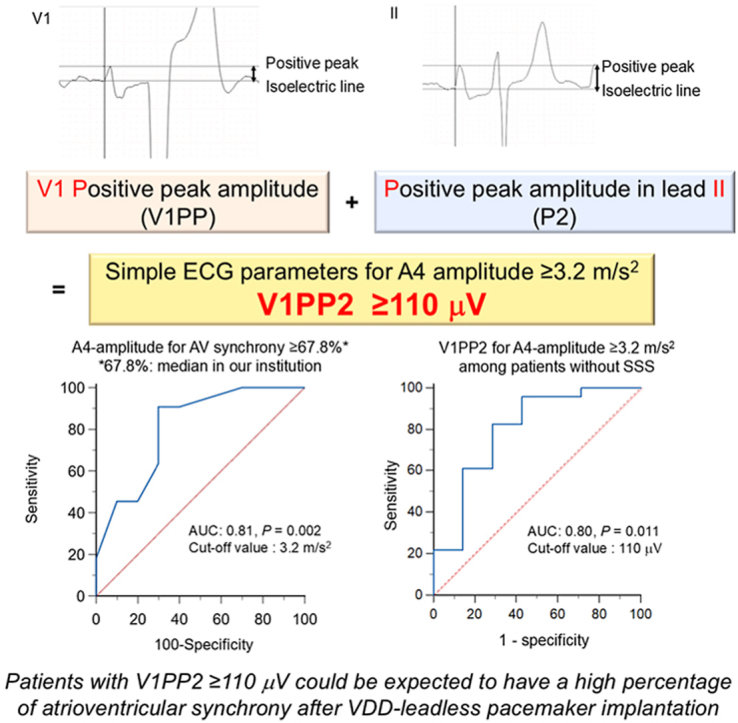
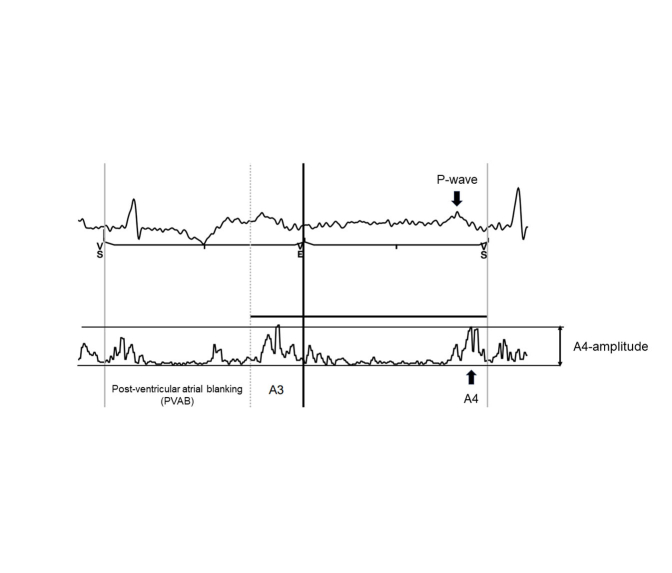
Background: A4-wave amplitude (A4-amplitude) is a crucial factor determining the percentage of atrioventricular synchrony (%AVS) in a mechanical sensing-based VDD leadless pacemaker (VDD-LP). We hypothesized that 12-lead electrocardiographic (ECG) parameters related to right atrial (RA) excitation could predict A4-amplitude.
Objectives: We aimed to investigate the relationship between A4-amplitude and 12-lead ECG parameters reflecting RA excitation and assess its predictive power for achieving an appropriate A4-amplitude associated with high %AVS.
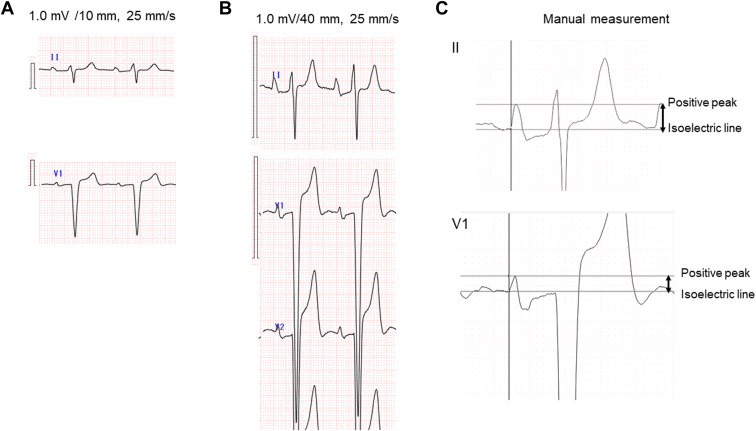
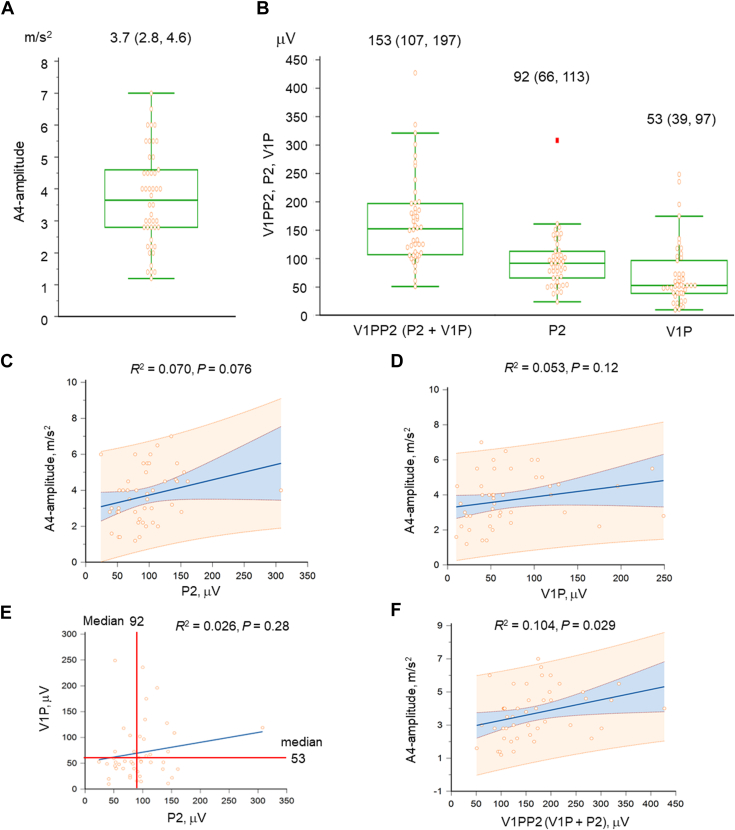
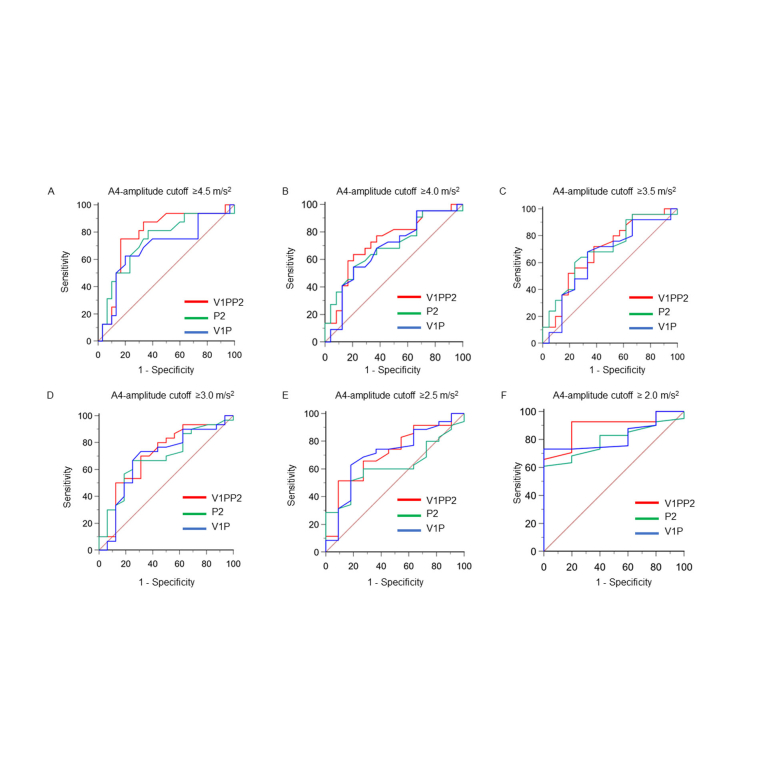
Methods: This single-center, retrospective, observational study enrolled consecutive patients undergoing VDD-LP implantation. The relationship between A4-amplitude and the positive peak amplitude of the P wave in lead II (P2), the positive peak amplitude of the P wave in lead V1 (V1P), and the sum of P2 and V1P (V1PP2) were assessed.
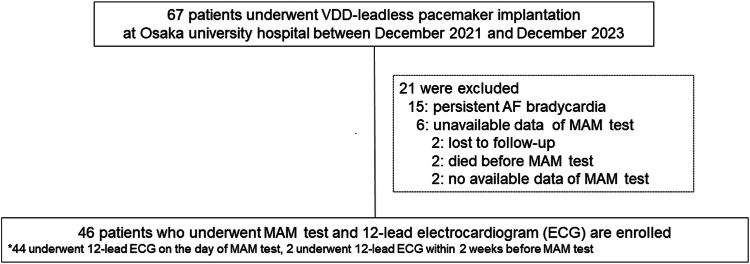
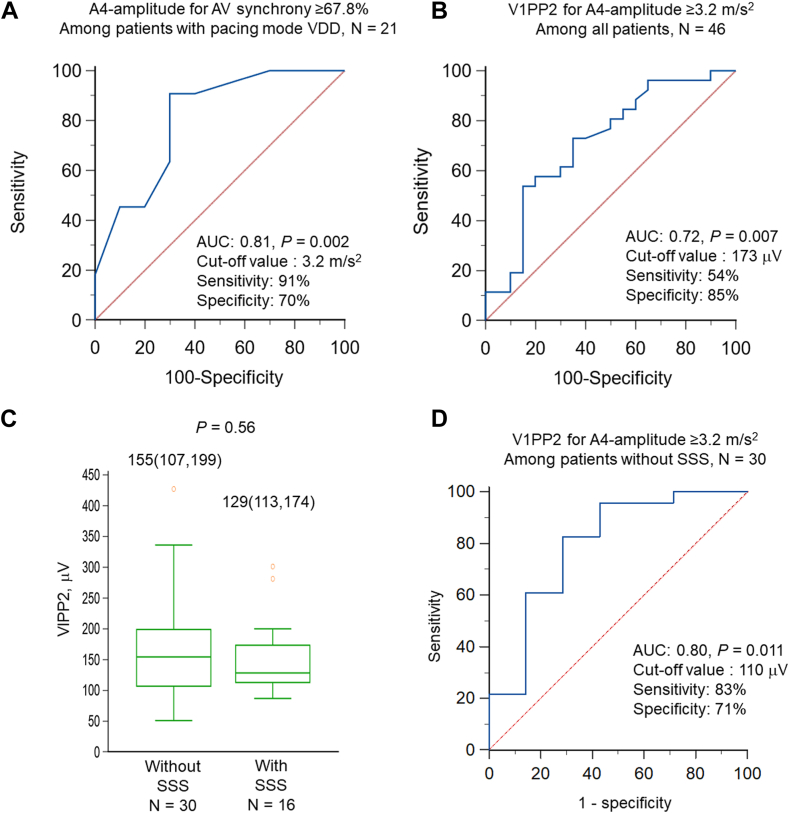
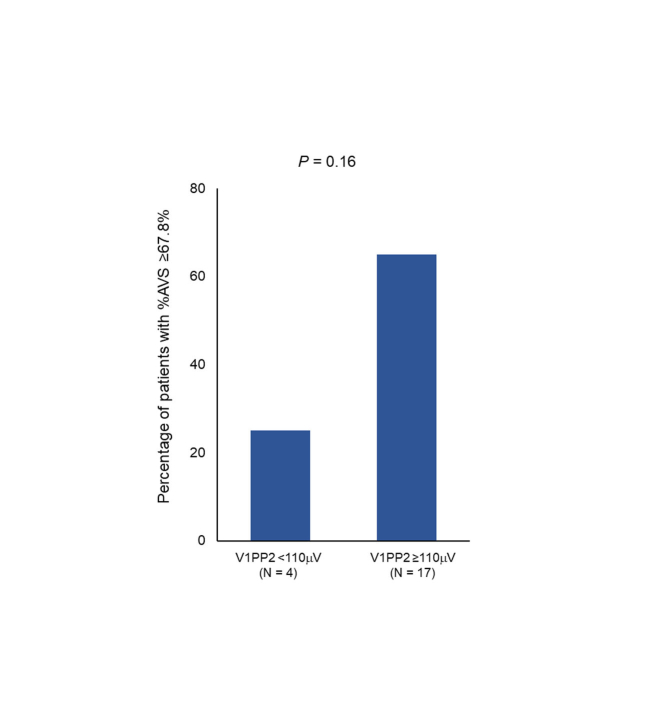
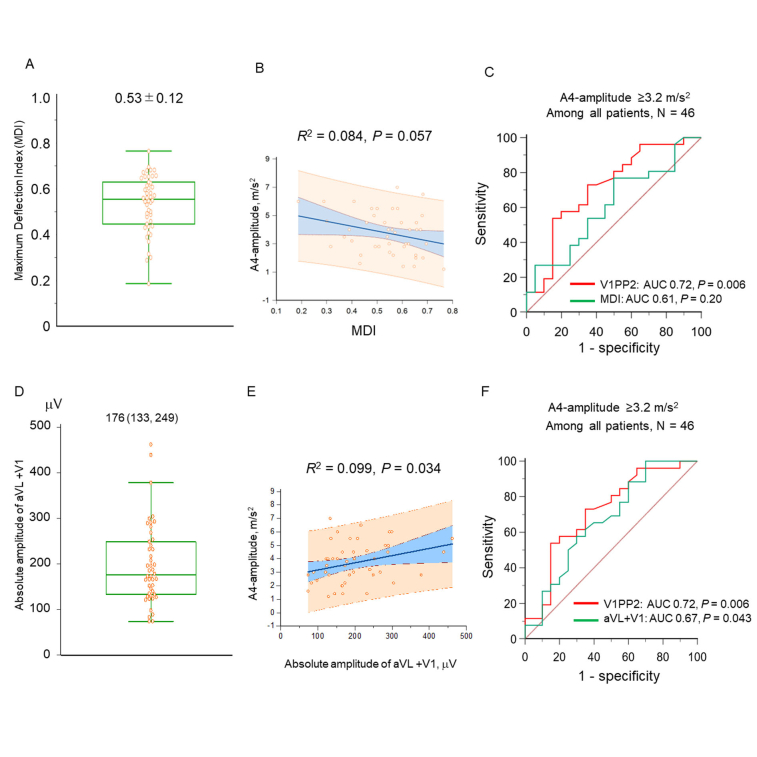
Results: Of the 67 patients undergoing VDD-LP implantation, 46 without atrial fibrillation bradycardia were enrolled. They had a data set of manual atrial mechanical sensing tests and 12-lead ECG. Among P2, V1P, and V1PP2, only V1PP2 was correlated with A4-amplitude (R 2=0.10; P=.029). In 30 patients in VDD pacing mode, the median %AVS was 67.8%. The A4-amplitude cutoff for %AVS ≥ 67.8% was 3.2 m/s2 (area under the curve [AUC] 0.81; P=.002). For A4-amplitude ≥ 3.2 m/s2, V1PP2 had moderate predictive power (AUC 0.72; P=.007). In 30 patients without sick sinus syndrome, the predictive power of V1PP2 for A4-amplitude ≥ 3.2 m/s2 was increased (AUC 0.80; cutoff value 110 μV; sensitivity 83%; specificity 71%; P=.011).
Conclusion: V1PP2, reflecting RA excitation, was related to A4-amplitude and had moderate predictive power. Notably, its predictive power increased when limited to patients without sick sinus syndrome. V1PP2 is a simple ECG predictor of A4-amplitude.
Keywords: 12-Lead electrocardiogram; Atrioventricular block; Atrioventricular synchrony; Leadless pacemaker; P-wave; Sick sinus syndrome.
© 2025 Heart Rhythm Society. Published by Elsevier Inc.
Figures
Similar articles
-
Electrocardiographic predictors of atrial mechanical sensing in leadless pacemakers.Heart Rhythm. 2024 Jul;21(7):1072-1080. doi: 10.1016/j.hrthm.2024.02.061. Epub 2024 Mar 1. Heart Rhythm. 2024. PMID: 38432424
-
Predictor of A4 amplitude using preprocedural electrocardiography in patients with leadless pacemakers.Heart Rhythm. 2024 Jul;21(7):1064-1071. doi: 10.1016/j.hrthm.2024.02.033. Epub 2024 Feb 19. Heart Rhythm. 2024. PMID: 38382683
-
Predictors of atrial mechanical sensing and atrioventricular synchrony with a leadless ventricular pacemaker: Results from the MARVEL 2 Study.Heart Rhythm. 2020 Dec;17(12):2037-2045. doi: 10.1016/j.hrthm.2020.07.024. Epub 2020 Jul 24. Heart Rhythm. 2020. PMID: 32717315 Clinical Trial.
-
Atrial mechanical contraction and ambulatory atrioventricular synchrony: Predictors from the OPTIVALL study.J Cardiovasc Electrophysiol. 2023 Sep;34(9):1904-1913. doi: 10.1111/jce.16016. Epub 2023 Jul 22. J Cardiovasc Electrophysiol. 2023. PMID: 37482952
-
Strategies to improve atrioventricular synchrony in patients with a Micra AV leadless pacemaker.Europace. 2024 Mar 1;26(3):euae060. doi: 10.1093/europace/euae060. Europace. 2024. PMID: 38449430 Free PMC article. Review.
References
-
- Chinitz L., Ritter P., Khelae S.K., et al. Accelerometer-based atrioventricular synchronous pacing with a ventricular leadless pacemaker: results from the Micra atrioventricular feasibility studies. Heart Rhythm. 2018;15:1363–1371. - PubMed
-
- Garweg C., Splett V., Sheldon T.J., et al. Behavior of leadless AV synchronous pacing during atrial arrhythmias and stability of the atrial signals over time—results of the MARVEL Evolve subanalysis. Pacing Clin Electrophysiol. 2019;42:381–387. - PubMed
-
- Steinwender C., Khelae S.K., Garweg C., et al. Atrioventricular synchronous pacing using a leadless ventricular pacemaker: results from the MARVEL 2 Study. JACC Clin Electrophysiol. 2020;6:94–106. - PubMed
-
- Saunders J.L., Calatayud J.B., Schulz K.J., Maranhao V., Gooch A.S., Goldberg H. Evaluation of ECG criteria for P-wave abnormalities. Am Heart J. 1967;74:757–765. - PubMed
-
- Kligfield P., Gettes L.S., Bailey J.J., et al. Recommendations for the standardization and interpretation of the electrocardiogram: part I: the electrocardiogram and its technology: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: endorsed by the International Society for Computerized Electrocardiology. Circulation. 2007;115:1306–1324. - PubMed
LinkOut - more resources
Full Text Sources
