

This is a preprint.
Severe long-term clinical sequelae among Sudan ebolavirus disease survivors 2 years post-infection
- PMID: 40321748
- PMCID: PMC12047994
- DOI: 10.21203/rs.3.rs-6325522/v1
Severe long-term clinical sequelae among Sudan ebolavirus disease survivors 2 years post-infection
Update in
-
Long-term clinical sequelae among Sudan ebolavirus disease survivors 2 years post-infection: a matched cohort study.BMC Med. 2025 Jul 18;23(1):432. doi: 10.1186/s12916-025-04271-z. BMC Med. 2025. PMID: 40682158 Free PMC article.
Abstract
Background: While long-term clinical sequelae following ebolavirus disease (EVD) due to Zaire ebolavirus (EBOV) strain has been characterized, this has not been explored for Sudan ebolavirus (SUDV) strain.
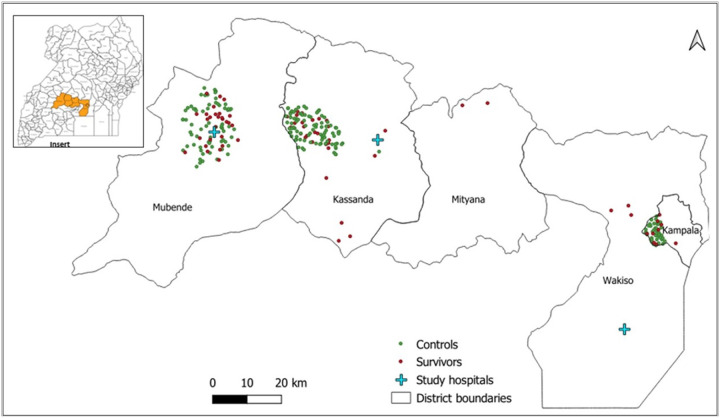
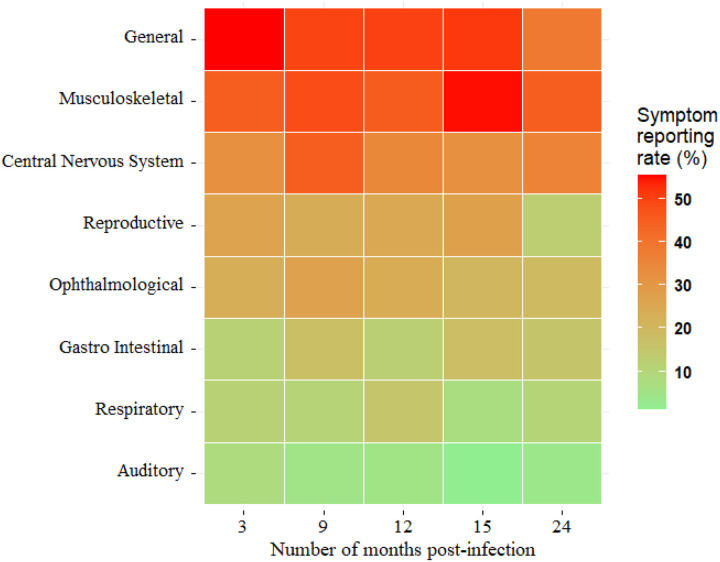
Methods: We enrolled 87 SUDV survivors from the 2022-2023 outbreak in Uganda, alongside 176 age-, sex-, and location-matched controls. Clinical symptom data were collected at 3-, 9-, 12-, 15-, and 18-and 24-months post-infection. Serum, semen, and breast milk samples were collected and tested for viral RNA.
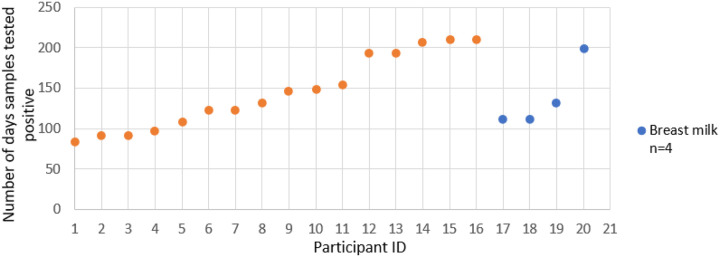
Results: Of 86 SUDV survivors, 57.5% reported significantly higher frequencies of clinical symptoms involving musculoskeletal (45.0%, P < 0.001), central nervous system (36.3%, p < 0.001), ophthalmologic (20%, P < 0.001), and respiratory (10%, P < 0.001) systems than those observed among controls. The risk ratio of occurrence was highest for ophthalmologic (20% vs 3.4%, RR = 5.9; p < 0.001) and central nervous systems symptoms (36.3% vs 6.8%, RR = 5.3, p < 0.001), and lowest for reproductive system (13.8% vs 8.5%; RR = 1.6; p > 0.005). Importantly, 50% of SUDV survivors reported persistent multi-systemic symptoms, including low back pain, hand and feet numbness, confusion, and diarrhoea that resulted in inability to perform basic activities of living. Viral RNA was detected in semen for a median duration of 131 days (range: 111-210 days) and in breast milk for a median of 149 days (range: 111-199 days).
Conclusions: This study demonstrates that SUDV survivors develop long-term clinical sequelae characterized by persistent multi-systemic clinical symptoms. Detection of viral RNA in semen and breastmilk for up to 7 months post-infection suggest prolonged persistence, with the possibility of latency and reactivation of the virus.
Conflict of interest statement
Competing interests The authors declare that they have no competing interests.
Figures
References
-
- Baize S, Pannetier D, Oestereich L, Rieger T, Koivogui L, Magassouba NF, et al. Emergence of Zaire Ebola Virus Disease in Guinea. New England Journal of Medicine. 2014;371(15):1418–25. - PubMed
-
- Izudi J, Bajunirwe F. Case fatality rate for Ebola disease, 1976–2022: A meta-analysis of global data. Journal of Infection and Public Health. 2024;17(1):25–34. - PubMed
-
- Tozay S, Fischer WA, Wohl DA, Kilpatrick K, Zou F, Reeves E, et al. Long-term Complications of Ebola Virus Disease: Prevalence and Predictors of Major Symptoms and the Role of Inflammation. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2020;71(7):1749–55. - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
