

Life-Saving Precision: Image-Guided Interventions Transforming Outcomes in Living-Donor Liver Transplant Complications
- PMID: 40322429
- PMCID: PMC12048113
- DOI: 10.7759/cureus.81613
Life-Saving Precision: Image-Guided Interventions Transforming Outcomes in Living-Donor Liver Transplant Complications
Abstract
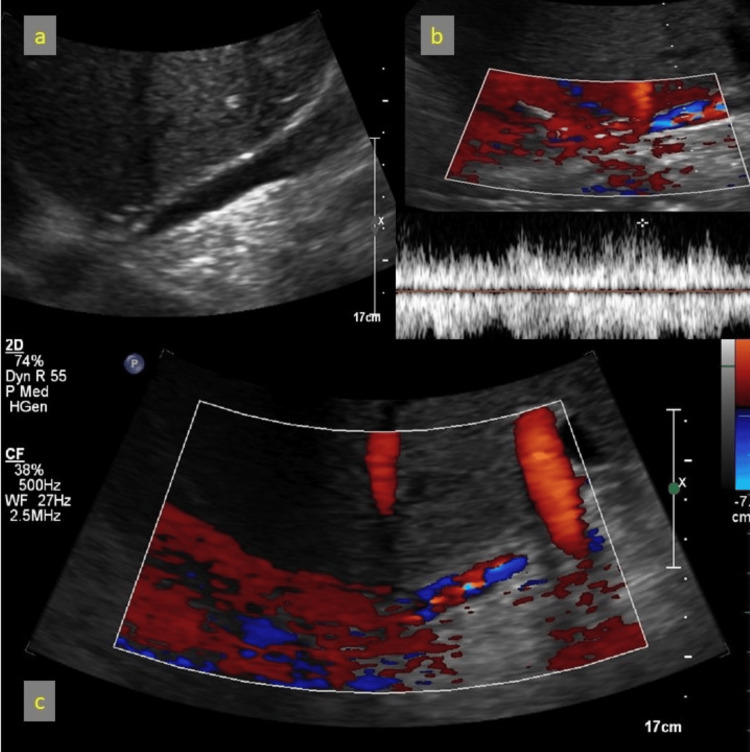
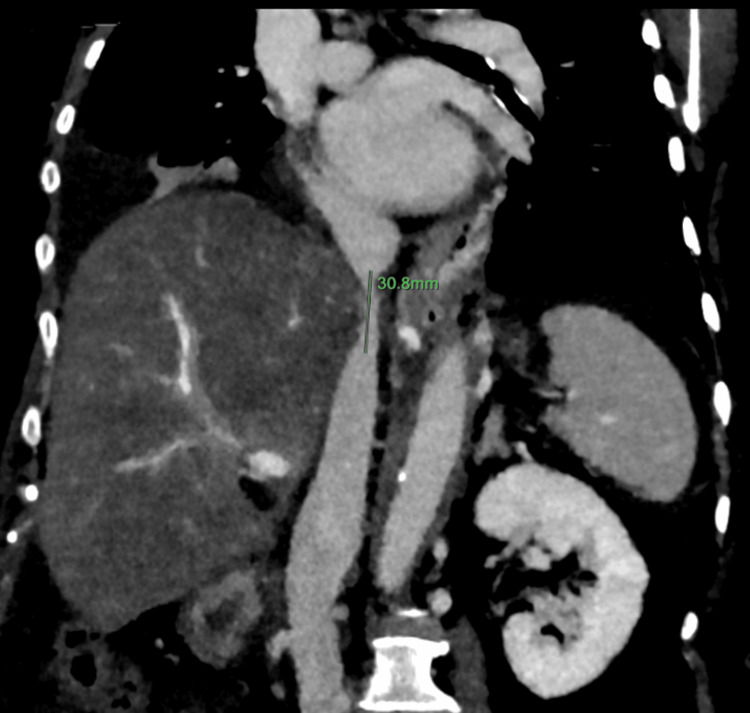
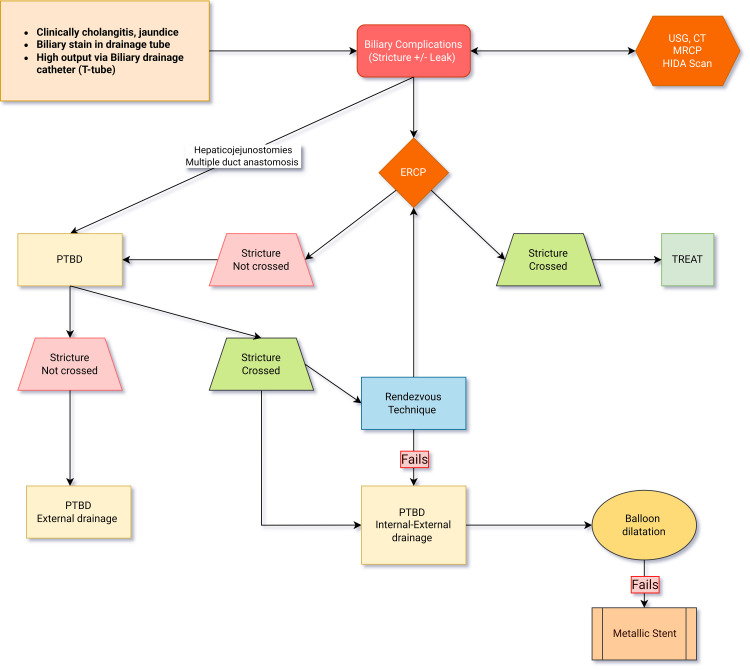
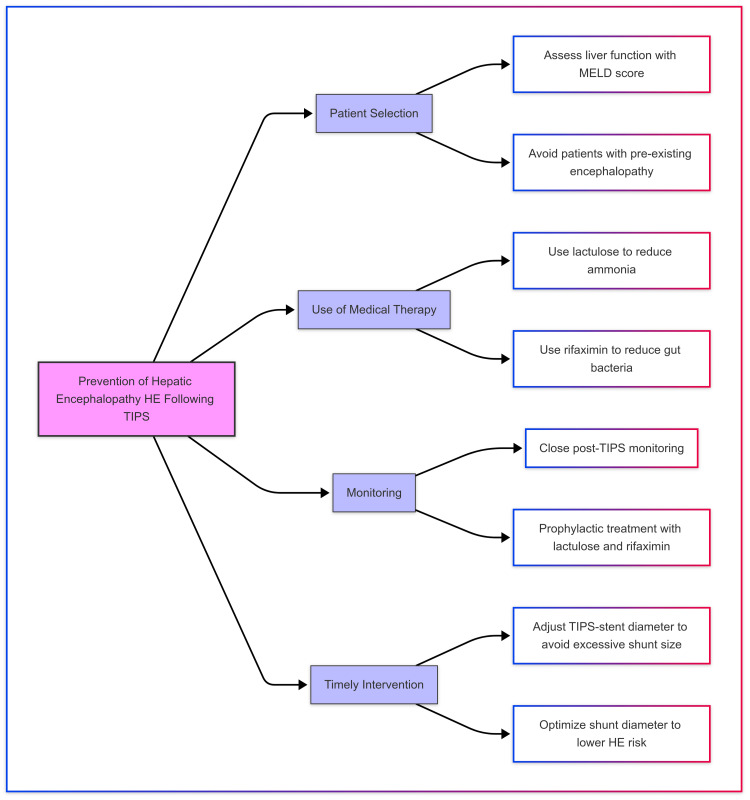
Living-donor liver transplantation (LDLT) is a preferred treatment modality for patients with end-stage liver disease. However, the incidence of postoperative complications, particularly involving the biliary and vascular systems, remains significant. These complications often necessitate urgent interventional management to prevent graft loss. Although surgical revision is an option, it carries increased morbidity and mortality risks. This case series explores the utility of minimally invasive, image-guided techniques for managing complex post-LDLT complications. We present four cases involving distinct image-guided interventions, including percutaneous transhepatic biliary drainage (PTBD) with balloon cholangioplasty for biliary strictures, hepatic venoplasty with intravascular stenting for hepatic venous outflow tract obstruction, and transjugular intrahepatic portosystemic shunt (TIPS) placement for refractory ascites secondary to portal hypertension. Procedural techniques, immediate outcomes, and follow-up results were assessed. All interventions were technically successful, with immediate clinical and biochemical improvement observed in each patient. Follow-up imaging confirmed patency and resolution of the vascular or biliary complications. This series underscores the efficacy of image-guided interventions as a safer alternative to surgical re-exploration in complex post-transplant cases. Image-guided interventions, including PTBD, venoplasty, and TIPS, offer robust management solutions for biliary and vascular complications in LDLT recipients, highlighting the role of interventional radiology in post-transplant care.
Keywords: biliary complications; hepatic venoplasty; image-guided interventions; interventional radiology; living-donor liver transplantation (ldlt); minimally invasive procedures; percutaneous transhepatic biliary drainage (ptbd); postoperative management; transjugular intrahepatic portosystemic shunt (tips); vascular complications.
Copyright © 2025, Bright et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures















Similar articles
-
Interventional Radiology Management of Adult Liver Transplant Complications.Radiographics. 2022 Oct;42(6):1705-1723. doi: 10.1148/rg.220011. Radiographics. 2022. PMID: 36190864
-
Bile leak following living donor liver transplantation: clinical efficacy of percutaneous transhepatic treatment.Liver Transpl. 2008 Aug;14(8):1142-9. doi: 10.1002/lt.21501. Liver Transpl. 2008. PMID: 18668647
-
Percutaneous Transhepatic Biliary Drainage for Biliary Stricture After Endotherapy Failure in Living Donor Liver Transplantation: A Single-Centre Experience from India.J Clin Exp Hepatol. 2019 Nov-Dec;9(6):684-689. doi: 10.1016/j.jceh.2019.03.004. Epub 2019 Mar 25. J Clin Exp Hepatol. 2019. PMID: 31889748 Free PMC article.
-
Imaging and Intervention in the Management of Vascular Complications Following Liver Transplantation.J Clin Exp Hepatol. 2023 Sep-Oct;13(5):854-868. doi: 10.1016/j.jceh.2023.03.010. Epub 2023 Mar 31. J Clin Exp Hepatol. 2023. PMID: 37693256 Free PMC article. Review.
-
Management issues in post living donor liver transplant biliary strictures.World J Hepatol. 2016 Apr 8;8(10):461-70. doi: 10.4254/wjh.v8.i10.461. World J Hepatol. 2016. PMID: 27057304 Free PMC article. Review.
References
-
- Long-term outcomes of stent placement inside the bile duct for biliary strictures after living donor liver transplantation. Nishikawa Y, Uza N, Hata K, et al. Liver Transpl. 2022;28:88–97. - PubMed
-
- Long-term outcome of percutaneous interventions for hepatic venous outflow obstruction after pediatric living donor liver transplantation: experience from a single institute. Yabuta M, Shibata T, Shibata T, et al. J Vasc Interv Radiol. 2013;24:1673–1681. - PubMed
-
- Treatment of hepatic venous outflow obstruction after piggyback liver transplantation. Wang SL, Sze DY, Busque S, Razavi MK, Kee ST, Frisoli JK, Dake MD. Radiology. 2005;236:352–359. - PubMed
Publication types
LinkOut - more resources
Full Text Sources