

Endoscopic findings of gallbladder lesions evaluated with image-enhanced endoscopy: A preliminary study using resected gallbladders
- PMID: 40322542
- PMCID: PMC12048906
- DOI: 10.1002/deo2.70136
Endoscopic findings of gallbladder lesions evaluated with image-enhanced endoscopy: A preliminary study using resected gallbladders
Abstract
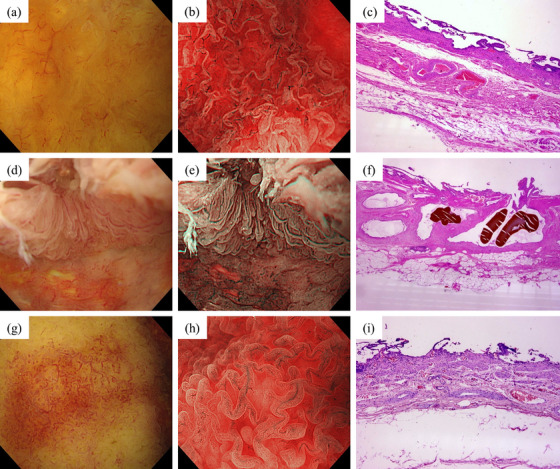
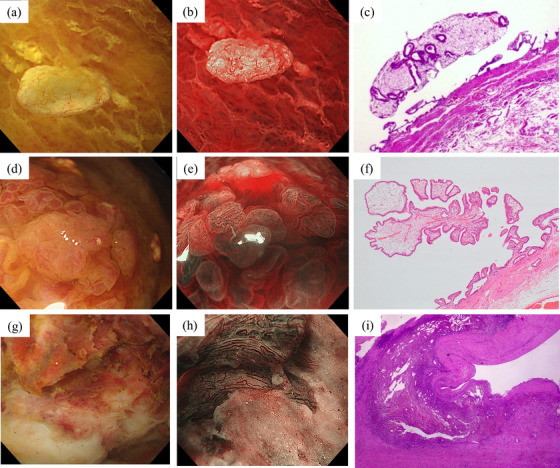
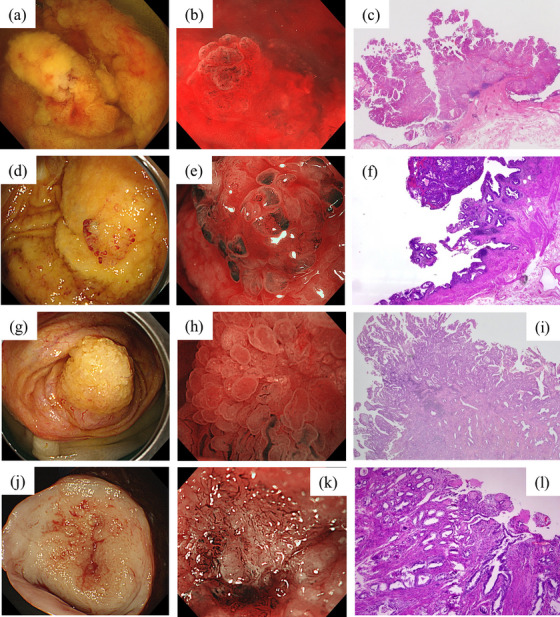
The diagnosis of gallbladder (GB) lesions relies on imaging findings. Transpapillary cholangioscopy can potentially be used to diagnose GB lesions; however, the images obtained remain unclear. This study aimed to characterize the endoscopic findings of GB lesions. We examined the endoscopic features of GB lesions in 50 consecutive patients who underwent cholecystectomy. GB specimens were obtained immediately following cholecystectomy, opened on the side opposite the liver bed, and flushed with saline solution. Each lesion was assessed using a high-resolution endoscope equipped with white light and narrow-band imaging magnification. For elevated lesions, both the surface structure (classified as regular, irregular, or absent) and vascular structure (dilation, meandering, caliber change, non-uniformity, and loose vessel areas) were assessed. Twelve of the 50 patients had elevated lesions, including cholesterol polyp (n = 4), hyperplastic polyp (n = 1), xanthogranulomatous cholecystitis (n = 1), and GB carcinoma (n = 6). Advanced GB carcinoma, as opposed to T1 GB carcinoma, demonstrated a papillary surface with destructive areas and neovascularization on narrow-band imaging magnification. Endoscopic images of each GB lesion were characterized, and the differences between GB carcinomas and benign lesions were identified. This preliminary classification may contribute to innovative imaging diagnosis and targeted biopsy for diagnosing GB lesions under direct vision.
Keywords: cholecystectomy; diagnosis; endoscopy; gallbladder; image‐enhanced endoscopy.
© 2025 The Author(s). DEN Open published by John Wiley & Sons Australia, Ltd on behalf of Japan Gastroenterological Endoscopy Society.
Conflict of interest statement
Hideki Kobara is an Associate Editor of DEN Open.
Figures
Similar articles
-
Can EUS-guided FNA distinguish between gallbladder cancer and xanthogranulomatous cholecystitis?Gastrointest Endosc. 2010 Sep;72(3):622-7. doi: 10.1016/j.gie.2010.05.022. Epub 2010 Jul 13. Gastrointest Endosc. 2010. PMID: 20630515
-
Combination of assay of human telomerase reverse transcriptase mRNA and cytology using bile obtained by endoscopic transpapillary catheterization into the gallbladder for diagnosis of gallbladder carcinoma.Am J Gastroenterol. 2003 Nov;98(11):2415-9. doi: 10.1111/j.1572-0241.2003.07693.x. Am J Gastroenterol. 2003. PMID: 14638342
-
Xanthogranulomatous cholecystitis: Difficulty in differentiating from gallbladder cancer.World J Gastroenterol. 2015 Sep 21;21(35):10166-73. doi: 10.3748/wjg.v21.i35.10166. World J Gastroenterol. 2015. PMID: 26401081 Free PMC article.
-
The Role of Endoscopic Ultrasound in the Diagnosis of Gallbladder Lesions.Diagnostics (Basel). 2021 Sep 28;11(10):1789. doi: 10.3390/diagnostics11101789. Diagnostics (Basel). 2021. PMID: 34679486 Free PMC article. Review.
-
[Recent Updates on Diagnosis, Treatment, and Follow-up of Gallbladder Polyps].Korean J Gastroenterol. 2020 Sep 25;76(3):102-107. doi: 10.4166/kjg.2020.76.3.102. Korean J Gastroenterol. 2020. PMID: 32969359 Review. Korean.
References
-
- Itoi T, Sofuni A, Itokawa F et al. Preoperative diagnosis and management of thick‐walled gallbladder based on bile cytology obtained by endoscopic transpapillary gallbladder drainage tube. Gastrointest Endosc 2006; 64: 512–9. - PubMed
-
- Sethi A, Tyberg A, Slivka A et al. Digital single‐operator cholangioscopy (DSOC) improves interobserver agreement (IOA) and accuracy for evaluation of indeterminate biliary strictures: The Monaco classification. J Clin Gastroenterol 2022; 56: e94–7. - PubMed
-
- Robles‐Medranda C, Valero M, Soria‐Alcivar M et al. Reliability and accuracy of a novel classification system using peroral cholangioscopy for the diagnosis of bile duct lesions. Endoscopy 2018; 50: 1059–70. - PubMed
-
- de Oliveira P, de Moura DTH, Ribeiro IB et al. Efficacy of digital single‐operator cholangioscopy in the visual interpretation of indeterminate biliary strictures: A systematic review and meta‐analysis. Surg Endosc 2020; 34: 3321–9. - PubMed
LinkOut - more resources
Full Text Sources