

Comparative Evaluation of Risk of Death in Mechanically Ventilated Patients With COVID-19 and Influenza: A Population-Based Cohort Study
- PMID: 40322716
- PMCID: PMC12045779
- DOI: 10.14740/jocmr6189
Comparative Evaluation of Risk of Death in Mechanically Ventilated Patients With COVID-19 and Influenza: A Population-Based Cohort Study
Abstract
Background: Reports on the comparative mortality among mechanically ventilated patients with coronavirus disease 2019 (COVID-19) and influenza show conflicting findings, but studies focused largely on the early phase of the pandemic, using historical influenza comparators. We sought to examine the population-level comparative mortality among mechanically ventilated patients with COVID-19 during the latter pandemic years using contemporaneous influenza comparators.
Methods: We used a statewide dataset to identify mechanically ventilated hospitalizations aged ≥ 18 years with COVID-19 or influenza in Texas between October 2021 and March 2023. Their comparative short-term mortality (in-hospital death or discharge to hospice) was estimated using overlap propensity score weighting (primary model), entropy balance, and hierarchical logistic models.
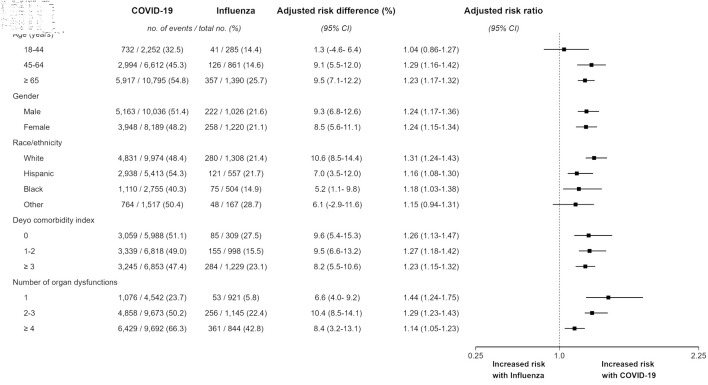
Results: Among 22,195 mechanically ventilated hospitalizations, 19,659 (88.6%) had COVID-19 and 2,536 (11.4%) had influenza. Compared to mechanically ventilated hospitalizations with influenza, those with COVID-19 were more commonly racial or ethnic minority (49.3% vs. 48.4%) and had lower mean (standard deviation (SD)) Deyo comorbidity index (2.04 (2.03) vs. 2.53 (1.91)), but higher number of organ dysfunctions (2.60 (1.37) vs. 2.13 (1.27)), respectively. Short-term mortality among mechanically ventilated hospitalizations with COVID-19 and influenza was 49.1% vs. 20.7%. The risk of short-term mortality was attenuated but remained higher among hospitalizations with COVID-19 in the primary model (adjusted risk ratio: 1.24 (95% confidence interval (CI): 1.18 - 1.30); adjusted risk difference 8.8% (95% CI: 6.7 - 10.4)), with consistent findings in alternative models, subgroups, and sensitivity analyses.
Conclusions: Population-level short-term mortality among mechanically ventilated hospitalizations with COVID-19 has been higher than that among those with influenza during the latter years of the pandemic.
Keywords: COVID-19; Influenza; Mechanical ventilation; Mortality.
Copyright 2025, Oud et al.
Conflict of interest statement
The authors declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
A Comparative Study on the Outcomes of Mechanically Ventilated COVID-19 vs Non-COVID-19 Patients with Acute Hypoxemic Respiratory Failure.Indian J Crit Care Med. 2021 Dec;25(12):1377-1381. doi: 10.5005/jp-journals-10071-24009. Indian J Crit Care Med. 2021. PMID: 35027797 Free PMC article.
-
Impact of history of mental disorders on short-term mortality among hospitalized patients with sepsis: A population-based cohort study.PLoS One. 2022 Mar 10;17(3):e0265240. doi: 10.1371/journal.pone.0265240. eCollection 2022. PLoS One. 2022. PMID: 35271683 Free PMC article.
-
Outcomes Among Mechanically Ventilated Patients With Severe Pneumonia and Acute Hypoxemic Respiratory Failure From SARS-CoV-2 and Other Etiologies.JAMA Netw Open. 2023 Jan 3;6(1):e2250401. doi: 10.1001/jamanetworkopen.2022.50401. JAMA Netw Open. 2023. PMID: 36626168 Free PMC article.
-
Corticosteroid treatment and mortality in mechanically ventilated COVID-19-associated acute respiratory distress syndrome (ARDS) patients: a multicentre cohort study.Ann Intensive Care. 2021 Nov 26;11(1):159. doi: 10.1186/s13613-021-00951-0. Ann Intensive Care. 2021. PMID: 34825976 Free PMC article.
-
In-hospital mortality, comorbidities, and costs of one million mechanically ventilated patients in Germany: a nationwide observational study before, during, and after the COVID-19 pandemic.Lancet Reg Health Eur. 2024 Jun 7;42:100954. doi: 10.1016/j.lanepe.2024.100954. eCollection 2024 Jul. Lancet Reg Health Eur. 2024. PMID: 39070745 Free PMC article.
References
-
- WHO COVID-19 Dashboard. World Health organization. Data. Available from: https://data.who.int/dashboards/covid19/deaths?n=o.
-
- COVID-1 Public Health Emergency. U.S. Department of Health and Human Services. Coronavirus. Available from: https://www.hhs.gov/coronavirus/covid-19-public-health-emergency/index.html.
-
- COVID Data Tracker. Centers for Disease Control and Prevention. Available from: https://covid.cdc.gov/covid-data-tracker/#trends_totaldeaths_select_00.
-
- Kojima N, Taylor CA, Tenforde MW, Ujamaa D, O'Halloran A, Patel K, Chai SJ. et al. Clinical outcomes of US adults hospitalized for COVID-19 and influenza in the respiratory virus hospitalization surveillance network, October 2021-September 2022. Open Forum Infect Dis. 2024;11(1):ofad702. doi: 10.1093/ofid/ofad702. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources