

Profiling of Anti-FVIII Antibodies in Acquired Haemophilia A: 'Insights into Domain Specificity, Isotype Variability, and Clinical Correlations'
- PMID: 40323009
- PMCID: PMC12311880
- DOI: 10.1111/hae.70056
Profiling of Anti-FVIII Antibodies in Acquired Haemophilia A: 'Insights into Domain Specificity, Isotype Variability, and Clinical Correlations'
Abstract
Introduction: Acquired haemophilia A (AHA) is a rare autoimmune disorder caused by autoantibodies against coagulation factor VIII (FVIII), resulting in significant bleeding risks.
Aim: To characterize the anti-FVIII antibody profile in AHA patients by assessing isotypes, subclasses, and correlations with key clinical parameters.
Methods: Eighty AHA patients were retrospectively analysed by assessing FVIII inhibitor levels, antibody isotypes (IgG, IgA, IgM), IgG subclasses, and domain specificity using a bead-based assay. Clinical data were correlated with antibody profiles. IgG domain profiles were compared with a congenital haemophilia A (CHA) cohort.
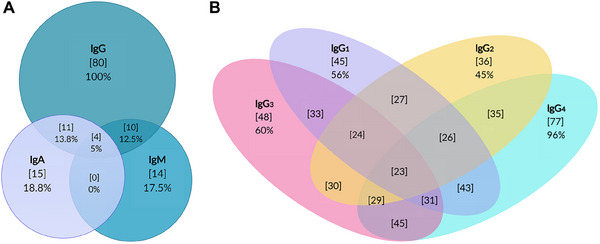
Results: The cohort had a median age of 74 years, with 60% males. Idiopathic cases accounted for 67%, and 17% had bleeding linked to medical interventions. Major bleeding sites were musculoskeletal/retroperitoneal (45%) and skin (36%). Within six months, 18% of patients died, mostly from sepsis. Anti-FVIII IgG antibodies were present in all patients, with IgG4 (96%) and IgG3 (60%) being the most common subclasses. IgM and IgA anti-FVIII antibodies were detected in 17.5% and 18.8% of patients, respectively, with IgM positivity associated with higher mortality (33%). IgG4 subclass correlated significantly with inhibitor titres (rs = 0.54; p < 0.001). Compared to CHA, AHA showed a higher prevalence of C1C2 domain-targeting antibodies (49% vs. 77%), associated with NBA levels (rs = 0.51; p < 0.001).
Conclusion: Anti-FVIII antibody profiling reveals distinct patterns in AHA, with IgG4 linked to higher inhibitor levels. The C1C2 domain specificity of the anti-FVIII antibodies suggests a potential role of this FVIII domain in the immunopathology of AHA patients, warranting further investigation to improve prognostic tools.
Keywords: FVIII inhibitors; acquired haemophilia A; anti‐FVIII antibodies; bleeding; immunoglobulin isotypes; mortality.
© 2025 The Author(s). Haemophilia published by John Wiley & Sons Ltd.
Conflict of interest statement
A.C.B. reports no conflicts of interest. I.M. and K.H. report no conflicts of interest. N.M. received grants/research supports/honoraria/consultation fees from: Bayer, Chugai, CSL Behring, LFB, NovoNordisk, Octapharma, Pfizer, Roche, Takeda and Sobi. T.A. reports having received grants for a patient support association from Bayer, Biotest, Chugai, CSL‐Behring, Grifols, Novo Nordisk, Octapharma, Roche, Swedish Orphan Biovitrum and Takeda, as well as personal fees for advisory board meetings, consulting and/or travel support from Bayer, Biomarin, Biotest, CSL‐Behring, Grifols, Novo Nordisk, Octapharma, Pfizer, Swedish Orphan Biovitrum and Takeda. J.O. reports having received grants for studies and research from Bayer, Biotest, CSL‐Behring, Octapharma, Pfizer, SOBI and Takeda, and travel support as well as personal fees for lectures and advisory board meetings from Bayer, Biogen Idec, Biomarin, Biotest, CSL‐Behring, Chugai, Freeline, Grifols, Novo Nordisk, Octapharma, Pfizer, Roche, Sanofi, Sparks, Swedish Orphan Biovitrum and Takeda. B.P. reports having received grants for research from Biotest and Octapharma as well as personal fees for lectures and advisory board meetings from NovoNordisk and Octapharma.
Figures

References
-
- Tiede A. and Wahler S., “The Rising Incidence of Acquired Haemophilia A in Germany,” Haemophilia: The Official Journal of the World Federation of Hemophilia 27, no. 4 (2021): e466–e468. - PubMed
-
- Verbruggen B., “Diagnosis and Quantification of Factor VIII Inhibitors,” Haemophilia: The Official Journal of the World Federation of Hemophilia 16, no. 102 (2010): 20–24. - PubMed
-
- Miller C. H., Payne A. B., Driggers J., Ellingsen D., Boylan B., and Bean C. J., “Reagent Substitutions in the Centers for Disease Control and Prevention Nijmegen‐Bethesda Assay for Factor VIII Inhibitors,” Haemophilia: The Official Journal of the World Federation of Hemophilia 24, no. 3 (2018): e116–e119. - PMC - PubMed
-
- Bonnefoy A., Merlen C., Dubé E., Claus‐Desbonnet H., Rivard G.‐E., and St‐Louis J., “Predictive Significance of Anti‐FVIII Immunoglobulin Patterns on Bleeding Phenotype and Outcomes in Acquired Hemophilia A: Results from the Quebec Reference Center for Inhibitors,” Journal of Thrombosis and Haemostasis JTH 19, no. 12 (2021): 2947–2956. - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
