

[Annual report 2025 from the National Database of the Regional Collaborative Rheumatology Centers in Germany]
- PMID: 40323420
- PMCID: PMC12605611
- DOI: 10.1007/s00393-025-01646-8
[Annual report 2025 from the National Database of the Regional Collaborative Rheumatology Centers in Germany]
Abstract
Background: Data of patients with inflammatory rheumatic diseases are annually recorded within the National Database of the German Collaborative Rheumatology Centers.
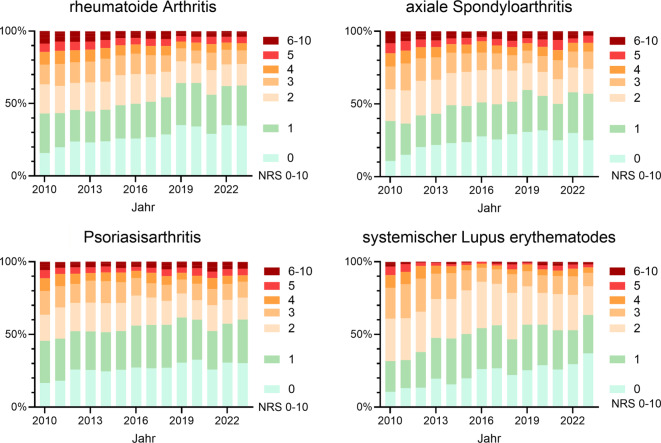
Methods: For rheumatoid arthritis (RA), psoriatic arthritis (PsA), axial spondylarthritis (axSpA), systemic lupus erythematosus (SLE), systemic sclerosis (SSc), Sjögren's syndrome (SjS), idiopathic inflammatory myositis (IIM), polymyalgia rheumatica (PMR), giant cell arteritis (GCA), ANCA-associated vasculitis (AAV), Behçet's disease (BD), adult onset Still's disease (AOSD) and autoinflammatory diseases (AID) data are reported from 2023. Information includes physician-reported disease activity on a numeric rating scale (NRS) of 0-10, treatment and patient-reported outcomes. For selected diagnoses, developments from 2010 to 2023 are presented regarding physicians' assessments of disease activity and treatment.
Results: A total of 13,884 patients were documented from 14 rheumatology centers, most frequently with RA (5734), PsA (1741) and axSpA (1494). The mean age ranged from 45 years (BD) to 73 years (GCA) and the median disease duration ranged from 3 years (PMR) to 16 years (axSpA). Disease activity was predominantly low, with 6% (BD) to 15% (axSpA) rated moderate to high (> 4 on the NMR) by rheumatologists. Biological disease-modifying antirheumatic drugs (bDMARD) were most frequently prescribed for axSpA (65%), AOSD (58%), PsA (53%) and GCA (41%). Tumor necrosis factor (TNF) inhibitors were frequently used in axSpA (53%), BD (30%) and PsA (28%), interleukin (IL)-1 inhibitors in AOSD (51%) and AID (50%), IL-6Ri in GCA (38%), IL17i in PsA (17%) and rituximab in AAV (29%). Higher levels of pain, fatigue, sleep disturbances and reduced well-being were reported by patients with IIM, SSc, axSpA and AID. Among those younger than 65 years, 58% (SSc) to 77% (axSpA) were employed. The percentage of early retirement due to rheumatic diseases was 5% (AOSD) to 18% (AAV). Since 2010 the development in the proportion of patients in remission or with very low disease activity (NRS 0-1) has increased across all diagnoses. In terms of treatment there has been an increase in b/tsDMARDs and a decrease in glucocorticoids for various diagnoses.
Conclusion: The results show the diversity of inflammatory rheumatic diagnoses and the continuously growing range of treatment in rheumatology along with good disease control in many patients.
Zusammenfassung: HINTERGRUND: Die Kerndokumentation der Regionalen Kooperativen Rheumazentren erfasst jährlich Versorgungsdaten von Patient:innen mit entzündlich rheumatischen Erkrankungen.
Methodik: Für rheumatoide Arthritis (RA), Psoriasisarthritis (PsA), axiale Spondyloarthritis (axSpA), systemischen Lupus erythematodes (SLE), systemische Sklerose (SSc), Sjögren-Syndrom (SjS), idiopathische inflammatorische Myositiden (IIM), Polymyalgia rheumatica (PMR), Riesenzellerarteriitis (RZA), ANCA-assoziierte Vaskulitiden (AAV), Morbus Behçet (BD), „adult-onset Still’s disease“ (AOSD) und autoinflammatorische Erkrankungen (AIE) werden Daten aus dem Jahr 2023 berichtet. Angaben umfassen u. a. die ärztlich eingeschätzte Krankheitsaktivität auf einer numerischen Ratingskala (NRS) von 0–10, Therapien und patientenberichtete Outcomes. Für ausgewählte Diagnosen werden Entwicklungen von 2010 bis 2023 zu der ärztlichen Einschätzung der Krankheitsaktivität und zu Therapien dargestellt.
Ergebnisse: Aus 14 Einrichtungen wurden 13.884 Patient:innen dokumentiert, am häufigsten RA (5734), PsA (1741) und axSpA (1494). Das mittlere Alter lag zwischen 45 (BD) und 73 Jahren (RZA), die Krankheitsdauer betrug im Median 3 (PMR) bis 16 Jahre (axSpA). Die Krankheitsaktivität war überwiegend niedrig, bei 6 % (BD) bis 15 % (axSpA) stuften die Rheumatolog:innen sie moderat bis hoch (> 4 auf numerischer Ratingskala) ein. Biologische (b)DMARDs wurden am häufigsten bei axSpA (65 %), AOSD (58 %), PsA (53 %) und RZA (41 %) verordnet. Häufig waren Tumornekrosefaktor(TNF)-Inhibitoren bei axSpA (53 %), BD (30 %) und PsA (28 %), Interleukin(IL)-1-Inhibitoren bei AOSD (51 %) und AIE (50 %), IL-6Ri bei RZA (38 %), IL-17i bei PsA (17 %) und Rituximab bei AAV (29 %). Höhere Einschränkungen hinsichtlich Schmerz, Fatigue, Schlafstörungen und Wohlbefinden dokumentierten v. a. Betroffene mit IIM, SSc, axSpA und AIE. Von den unter 65-Jährigen waren 58 % (SSc) bis 77 % (axSpA) erwerbstätig. Eine Berentung wegen der rheumatischen Erkrankung hatten 5 % (AOSD) bis 18 % (AAV). In der Entwicklung seit 2010 ist der Anteil an Patienten in Remission oder sehr niedriger Krankheitsaktivität (NRS 0–1) diagnoseübergreifend gestiegen. Bei den Therapien sind ein Anstieg an b/tsDMARDs und ein Rückgang von Glukokortikoiden bei verschiedenen Diagnosen sichtbar.
Schlussfolgerung: Die Ergebnisse zeigen die Vielfältigkeit der entzündlich rheumatischen Diagnosen und das kontinuierlich wachsende Therapiespektrum in der Rheumatologie, einhergehend mit einer guten Krankheitskontrolle bei vielen Patient:innen.
Keywords: DMARD therapy; Health services research; Long-term observational research; Rheumatic diseases; Rheumatology.
© 2025. The Author(s).
Conflict of interest statement
Einhaltung ethischer Richtlinien. Interessenkonflikt: J. Callhoff erhielt Referentenhonorare von Janssen, Pfizer und Idorsia. Tobias Alexander erhielt in den letzten 3 Jahren Honorare für Advisory Boards und/oder Vorträge von AbbVie, Amgen, AstraZeneca, GSK und Lilly. Martin Aringer erhielt Honorare für Advisory Boards und/oder Vorträge von AbbVie, AstraZeneca, BMS, Chugai, Galapagos, GSK, Lilly, MSD, Novartis, Roche, Sanofi und UCB. J. Detert erhielt Advisory Board- und Vortragshonorare von AbbVie, Amgen, BMS, Eli Lilly, Galapagos, Gilead, Janssen, Novartis, Pfizer und UCB. Martin Feuchtenberger erhielt Honorare für Advisory Boards und/oder Vorträge von AbbVie, Lilly, MSD, Novartis, Pfizer, Celltrion und UCB. J. Henes erhielt Vortragshonorare für AbbVie, AstraZeneca, Boehringer Ingelheim, BMS, Janssen, Lilly, Novartis, Pfizer, Roche, SOBI, Otsuka, EUSA und UCB. K. Karberg erhielt Vortragshonorare von AbbVie, UCB, Novartis und der Rheumaakademie. U. Kiltz erhielt Vortrags‑/Beratungshonorare von AbbVie, Amgen, Biocad, Biogen, Chugai, Eli Lilly, Fresenius, Gilead, Grünenthal, GSK, Janssen, MSD, Novartis, Pfizer, Roche und UCB. B. Köhler erhielt Vortragshonorare von AbbVie, Lilly und Novartis, Beratungshonorare von AbbVie, Amgen, Lilly, Pfizer, UCB und Unterstützung für Kongressreisen/-teilnahme von UCB, Pfizer, Lilly und AbbVie. Susanna Späthling-Mestekemper erhielt Vortrags‑/Beraterhonorare von AbbVie, AstraZeneca, BMS, Gilead, Grünenthal, GSK, Janssen, Lilly, MSD, Novartis, Pfizer, UCB. M. Steinmüller erhielt Vortrags‑/Beratungshonorare von AbbVie, Amgen, Berlin Chemie, BMS, Galapagos, Gilead, GSK, Janssen, Lilly, Medac, MSD, Mylan, Novartis, Pfizer und ViiV. A. Strangfeld erhielt Referentenhonorare von AbbVie, Biogen, Galapagos, Janssen, Lilly, Pfizer und Takeda. K. Albrecht, T. Eidner, A. Krause, J. Richter und K. Thiele geben an, dass bzgl. der Kerndokumentation keine Interessenkonflikte bestehen. Für die Studie liegt ein positives Ethikvotum von der Charité-Universitätsmedizin Berlin vor (EA1/196/06 und EA1/093/24). Alle Patient:innen haben bei Teilnahme an der Kerndokumentation ihr schriftliches Einverständnis gegeben.
Figures

References
-
- Albrecht K, Callhoff J, Zink A (2019) Langzeittrends in der rheumatologischen Versorgung : Erfolge und Defizite im Spiegel von 25 Jahren rheumatologischer Kerndokumentation. (Long-term trends in rheumatology care : Achievements and deficits in 25 years of the German national rheumatology database). Z Rheumatol 78(8):703–712. 10.1007/s00393-019-0660-5 - PubMed
-
- Thiele K, Albrecht K, Zink A, Aringer M, Karberg K, Spathling-Mestekemper S, von Hinuber U, Callhoff J (2022) Is the Rheumatoid Arthritis Impact of Disease (RAID) score a meaningful instrument for other inflammatory rheumatic diseases? A cross-sectional analysis of data from the German National Database. RMD Open. 10.1136/rmdopen-2022-002342 - PMC - PubMed
-
- Thiele K, Albrecht K, Alexander T, Aringer M, Detert J, Eidner T, Feuchtenberger M, Henes J, Karberg K, Kiltz U, Köhler B, Krause A, Richter JG, Späthling-Mestekemper S, Steinmüller M, Zinke S, Callhoff J (2025) Kerndokumentation der regionalen kooperativen Rheumazentren. Versorgungstrends 2025. 10.17169/refubium-46216
-
- Veltri C, Albrecht K, Kiltz U, Meyer-Olson D, Spathling S, Strangfeld A, Thiele K, Callhoff J (2025) Trends in work participation among patients with inflammatory rheumatic musculoskeletal diseases (iRMDs): Data from the German National Database (2010–2022). Rmd Open. 10.1136/rmdopen-2024-004980 - PMC - PubMed
-
- Steffen A, Holstiege J, Klimke K, Akmatov MK, Batzing J (2018) Patterns of the initiation of disease-modifying antirheumatic drugs in incident rheumatoid arthritis: a German perspective based on nationwide ambulatory drug prescription data. Rheumatol Int 38(11):2111–2120. 10.1007/s00296-018-4161-7 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
