

Predictors of response to burosumab in adults with X-linked hypophosphatemia: real-world data from an Italian cohort
- PMID: 40323576
- PMCID: PMC12313718
- DOI: 10.1007/s40618-025-02596-3
Predictors of response to burosumab in adults with X-linked hypophosphatemia: real-world data from an Italian cohort
Abstract
Purpose: X-linked hypophosphatemia (XLH) is a genetic disorder characterized by elevated FGF23 levels, leading to phosphate wasting and hypophosphatemia, causing skeletal and extraskeletal abnormalities. Burosumab, an antibody targeting FGF23, improves hypophosphatemia and clinical outcomes. This study evaluated the real-world efficacy of burosumab and identify predictors of treatment response.
Methods: Twenty-seven adult XLH patients (mean age 42 years; 48% female) from an Italian multicenter cohort were treated with burosumab for up to 24 weeks. Laboratory tests were evaluated at midpoints and endpoints (14 and 28 days) of the dosing interval. In a subset of patients (N = 11) followed for 48 weeks, laboratory tests and patient-reported outcomes were also assessed.
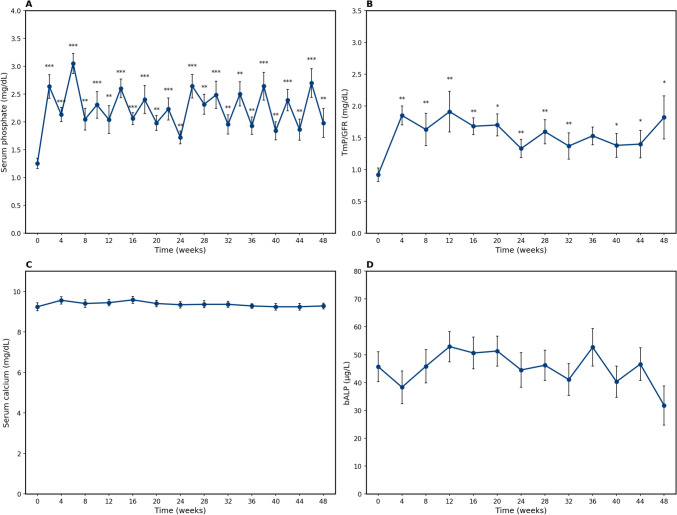
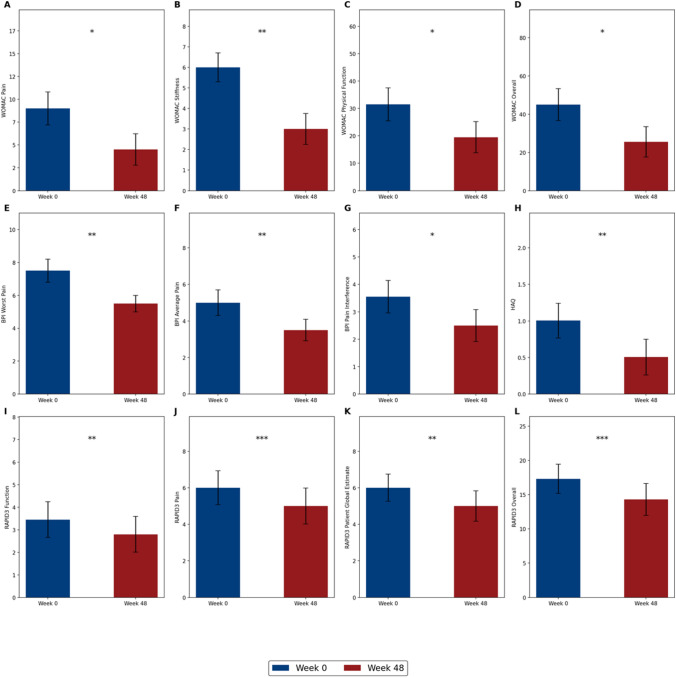
Results: After initiating burosumab, median serum phosphate levels increased from 1.5 mg/dL (IQR 1.3-1.8) to 2.0 mg/dL (IQR 1.7-2.4) (p < 0.05), remaining higher than baseline at the midpoints of the dosing interval for up to 24 weeks. Higher baseline phosphate predicted higher midpoint levels (p < 0.05), whereas higher baseline PTH (p < 0.05) and FGF23 (p < 0.001) were associated with lower phosphate levels at midpoints. In patients (N = 11) followed for 48 weeks, significant improvements in patient-reported outcomes in all patients were observed. Both WOMAC Pain (r = 0.94, p = 0.02) and BPI Worst Pain (r = 0.98, p < 0.001) were positively correlated with increased phosphate at week 48.
Conclusion: Burosumab effectively increased serum phosphate levels and improved clinical outcomes in a real-world setting, particularly in patients with more substantial increases in serum phosphate levels. Baseline serum phosphate, PTH, and FGF23 levels predicted response, helping tailor treatment strategies and improve long-term patient management.
Keywords: Burosumab; FGF23; Patient-reported outcomes; Real-life; Serum phosphate; X-linked hypophosphatemia.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: GM: Kyowa Kirin consultation. All other authors have no conflict of interest to declare. Ethical approval: This study was performed in accordance with the 1964 Helsinki declaration and its later amendments and was authorized by the Ethics Committee (Comitato Etico Territoriale Area Centro-Est Veneto, 391n/AO/23). The committee provided ethical approval for the research protocol, ensuring that the study complies with the ethical standards for research involving human participants. Informed consent: All participants provided written informed consent to their participation after being informed about the study’s nature and purpose.
Figures

References
-
- Laurent MR, Harvengt P, Mortier GR, Böckenhauer D (1993) X-Linked Hypophosphatemia. In: Adam MP, Feldman J, Mirzaa GM, et al (eds) GeneReviews®. University of Washington, Seattle, Seattle (WA) - PubMed
-
- Francis F, Hennig S, Korn B et al (1995) A gene (PEX) with homologies to endopeptidases is mutated in patients with X–linked hypophosphatemic rickets. Nat Genet 11:130–136. 10.1038/ng1095-130 - PubMed
-
- Kamenický P, Briot K, Munns CF, Linglart A (2024) X-linked hypophosphataemia. Lancet Lond Engl 404:887–901. 10.1016/S0140-6736(24)01305-9 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
