

Efficacy of vitrectomy combined with and without cataract surgery for diabetic macular edema: one-year follow-up multi-center study in Japan
- PMID: 40327087
- PMCID: PMC12513882
- DOI: 10.1007/s00417-025-06845-2
Efficacy of vitrectomy combined with and without cataract surgery for diabetic macular edema: one-year follow-up multi-center study in Japan
Abstract
Purpose: To evaluate the efficacy of vitrectomy, with and without cataract surgery, for diabetic macular edema (DME) in Japan.
Method: This retrospective study was conducted at 22 sites in Japan and enrolled patients who underwent vitrectomy either without (VIT group) or with (VIT + CS group) cataract surgery. Central retinal thickness (CRT) and best-corrected visual acuity (BCVA) were measured before surgery and at 1, 3, 6, and 12 months after surgery.
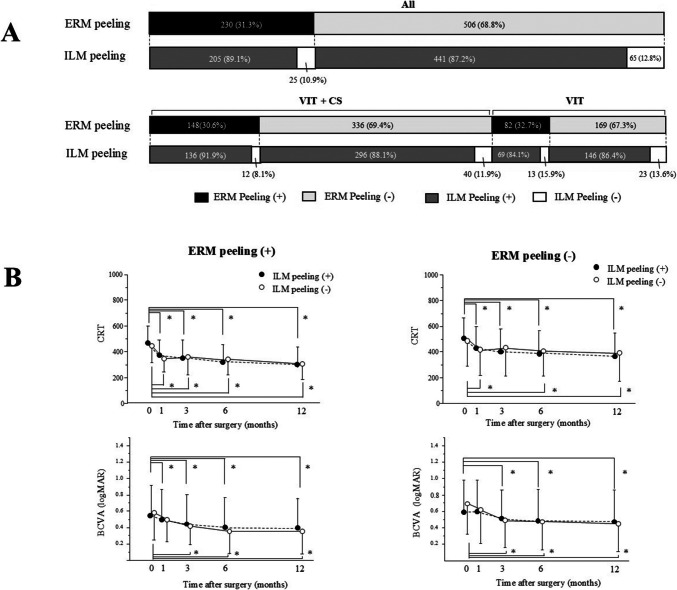
Results: A total of 722 patients with DME (482 in the VIT + CS group and 240 in the VIT group) were enrolled. CRT significantly decreased after 1 month and continued thereafter in both groups. BCVA significantly improved at 1 month in the VIT + CS group and at 6 months in the VIT group. In both groups, regardless of epiretinal membrane removal, CRT and BCVA significantly improved, with no additional benefit from concomitant internal limiting membrane peeling. The change in BCVA was significantly correlated with the change in CRT during 6 months postoperatively in all patients and in the VIT group. Patients with worse preoperative visual acuity had a higher likelihood of improved BCVA at 6 and 12 months after surgery. No significant difference in BCVA was observed before and after surgery in patients with a preoperative visual acuity of 20/40 or better. However, in patients with a visual acuity of 20/50 or worse, BCVA significantly improved 1 month after surgery.
Conclusion: Vitrectomy is anatomically and functionally effective for DME, and combined cataract surgery is beneficial in DME cases with cataracts. Patients with poor preoperative BCVA improved, while those with good vision maintained it. However, better preoperative vision increased the risk of postoperative deterioration, underscoring the need for careful evaluation of surgical indications.
Key messages: What is known In vitrectomy for diabetic macular edema (DME), DRCR.net showed that 13-31% of patients experience decreased vision despite reduced edema, leaving the efficacy of vitrectomy uncertain. What is new Our multicenter study demonstrated that vitrectomy with and without cataract surgery was effective in improving central retinal thickness and visual acuity in the patients with DME. Better preoperative visual acuity increased the risk of postoperative decline, and thus the need for careful evaluation of surgical indications.
Keywords: Cataract surgery; Diabetic macular edema; Epiretinal membrane; Vitrectomy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: Our protocol was approved by the Institutional Review Board (IRB) of the University of Fukui, No 20230129. Informed consent: This study used an opt-out approach. Participants were provided with information about the study, including its objectives and the use of their data and were given the opportunity to decline participation. Human and animal rights: All procedures involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Conflict of interest: All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interests; expert testimony or patent-licensing arrangements) or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
Figures




References
-
- Terasaki H, Ogura Y, Kitano S et al (2018) Management of diabetic macular edema in Japan: a review and expert opinion. Jpn J Ophthalmol 62:1–23. 10.1007/s10384-017-0537-6 - PubMed
-
- Ogura Y, Shiraga F, Terasaki H et al (2017) Clinical practice pattern in management of diabetic macular edema in Japan: survey results of Japanese retinal specialists. Jpn J Ophthalmol 61:43–50. 10.1007/s10384-016-0481-x - PubMed
-
- Parikh R, Ross JS, Sangaralingham LR et al (2017) Trends of Anti-Vascular Endothelial Growth Factor Use in Ophthalmology Among Privately Insured and Medicare Advantage Patients. Ophthalmology 124:352–358. 10.1016/j.ophtha.2016.10.036 - PubMed
-
- Tachi N, Ogino N (1996) Vitrectomy for diffuse macular edema in cases of diabetic retinopathy. Am J Ophthalmol 122:258–260. 10.1016/S0002-9394(14)72018-5 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
