

Atypical causes of respiratory virus infections in Sub-Saharan Africa from 2013- 2023: a systematic review and meta-analysis
- PMID: 40329172
- PMCID: PMC12057230
- DOI: 10.1186/s12879-025-11028-9
Atypical causes of respiratory virus infections in Sub-Saharan Africa from 2013- 2023: a systematic review and meta-analysis
Abstract
Background: Atypical respiratory viruses (ARVs) are a diverse group of pathogens that cause respiratory infections through less common mechanisms or in unique epidemiological patterns, unlike the typical viruses like respiratory syncytial virus, influenza and human rhinoviruses. They sometimes present as unusual respiratory illnesses in vulnerable populations with near-fatal outcomes. Several viruses are involved, such as Human metapneumovirus (HMPV), Human Bocavirus (HBoV), Enteroviruses (EVs), Parechovirus (PeV) and Influenza C virus (ICV). This review was done to shed light on ARVs and their possible role in respiratory illness or infections based on studies in Sub-Saharan Africa from 2013 to 2023.
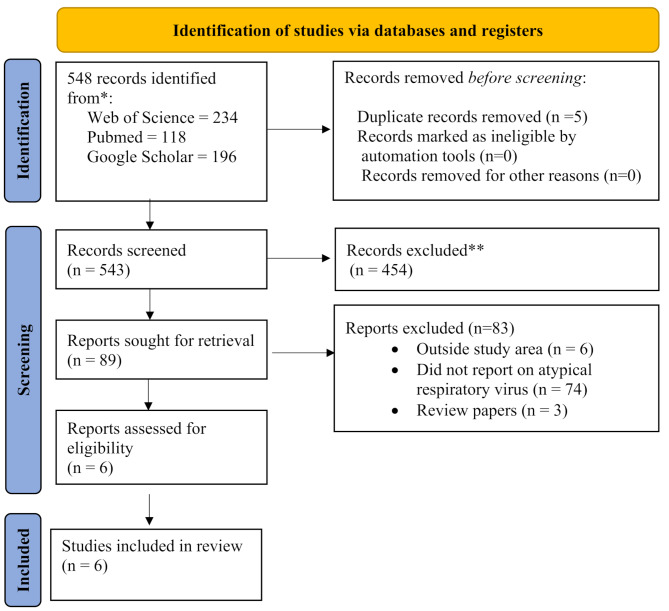
Methods: We systematically reviewed atypical causes of respiratory virus infections in Sub-Saharan Africa (SSA) in line with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 guidelines. We searched PubMed, Web of Science, Google Scholar and Cochrane Library to include studies published from 2013 to 2023 with reports on ARV. The protocol was registered in PROSPERO (ID: CRD42024611183).
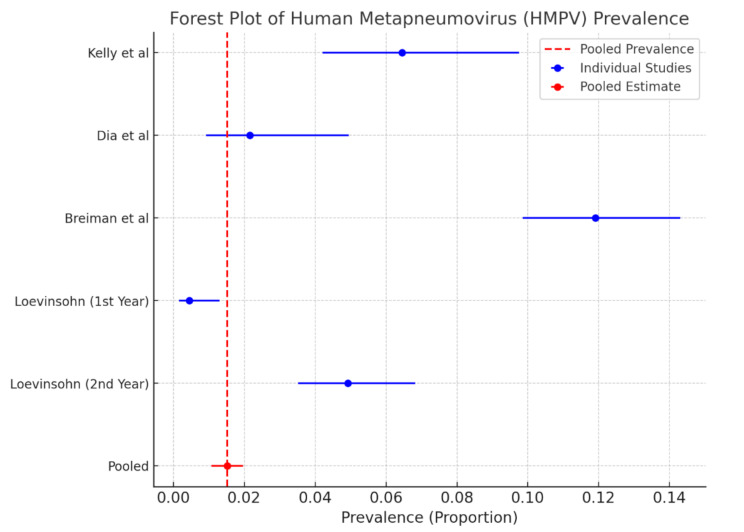
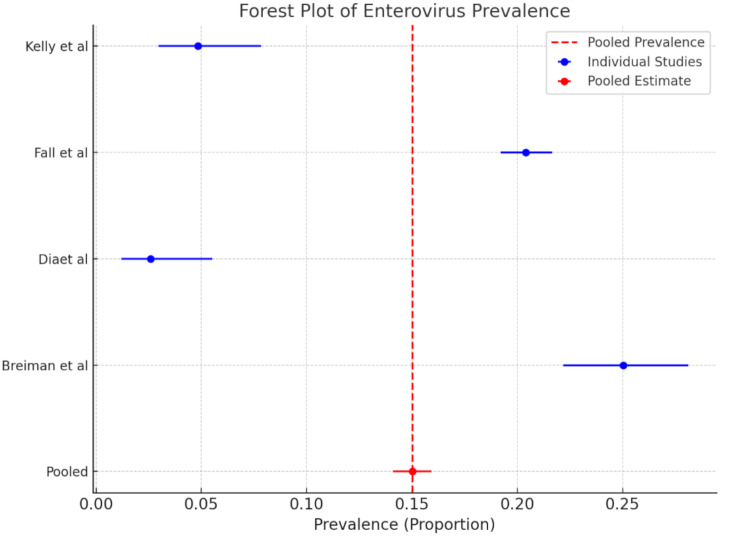
Results: The review covered 46 SSA countries, with five eligible for the systematic review. The search yielded 548 publications, with only six studies meeting the inclusion criteria. Studies included children and individuals of all age groups. The prevalence of ARVs detected in SSA was as follows: HMPV pooled prevalence was 1.52% (95% CI: 1.07-2.00), EVs pooled prevalence was 15.0% (95% CI: 14.1-15.9), HBoV prevalence was 0.4%, PeV was 20%, and ICV was 1.3% in individuals with respiratory tract infection(s).
Conclusion: Our findings suggest testing or diagnostics for ARV infections are very low in SSA. Therefore, surveillance of people suffering from respiratory tract infections, which is lacking, needs to be improved to monitor the prevalence of ARVs and the role they play in respiratory disease outcomes.
Keywords: Atypical respiratory viruses; Diagnostic methods; Prevalence; Sub-Saharan Africa.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Clinical trial number: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Contribution of common and recently described respiratory viruses to annual hospitalizations in children in South Africa.J Med Virol. 2011 Aug;83(8):1458-68. doi: 10.1002/jmv.22120. J Med Virol. 2011. PMID: 21678450 Free PMC article.
-
Molecular epidemiology of influenza, RSV, and other respiratory infections among children in Qatar: A six years report (2012-2017).Int J Infect Dis. 2020 Jun;95:133-141. doi: 10.1016/j.ijid.2020.04.008. Epub 2020 Apr 9. Int J Infect Dis. 2020. PMID: 32278934 Free PMC article.
-
Increased risk during winter: common respiratory viruses and clinical outcomes in hospitalized children.BMC Infect Dis. 2025 Apr 19;25(1):563. doi: 10.1186/s12879-025-10950-2. BMC Infect Dis. 2025. PMID: 40253326 Free PMC article.
-
Prevalence of metabolic syndrome among people living with human immunodeficiency virus in sub-Saharan Africa: a systematic review and meta-analysis.Sci Rep. 2024 May 22;14(1):11709. doi: 10.1038/s41598-024-62497-y. Sci Rep. 2024. PMID: 38777850 Free PMC article.
-
Etiology of acute viral respiratory infections common in Pakistan: A review.Rev Med Virol. 2019 Mar;29(2):e2024. doi: 10.1002/rmv.2024. Epub 2018 Dec 12. Rev Med Virol. 2019. PMID: 30548740 Free PMC article.
References
-
- Shaw T, Indumathi VA. The viral etiologies of severe acute respiratory infection: Indian perspective on the emerging pathogens. J Pure Appl Microbiol. 2020;14(4):2277–85.
-
- Jartti T, Jartti L, Ruuskanen O, Söderlund-Venermo M. New respiratory viral infections. Curr Opin Pulm Med. 2012;18(3):271–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
