

Early norepinephrine for patients with septic shock: an updated systematic review and meta-analysis with trial sequential analysis
- PMID: 40329359
- PMCID: PMC12057179
- DOI: 10.1186/s13054-025-05400-z
Early norepinephrine for patients with septic shock: an updated systematic review and meta-analysis with trial sequential analysis
Abstract
Background: The optimal timing for initiating norepinephrine in septic shock is debated. This updated systematic review and meta-analysis aimed to evaluate the impact of early versus delayed norepinephrine initiation on mortality and clinical outcomes in adults with septic shock.
Methods: A systematic search in Pubmed, EMbase and the Cochrane Library to identify eligible randomized controlled trials, propensity score matching (PSM) and observational studies that compare early norepinephrine initiation with non-early norepinephrine initiation in patients with acute circulatory failure. The primary outcome was mortality in intensive care unit. Secondary outcomes included intensive care unit length of stay, fluid volume received at 6 h, norepinephrine dose, mechanical ventilation-free days, renal replacement therapy free days, and time to achieve a targeted mean arterial pressure (MAP). Meta-analysis and subgroup analysis were conducted to calculate odds ratio (OR) or mean difference with 95% confidence interval (95%CI) using random-effect model. Trial sequential analysis was conducted to evaluate the conclusiveness of evidence.
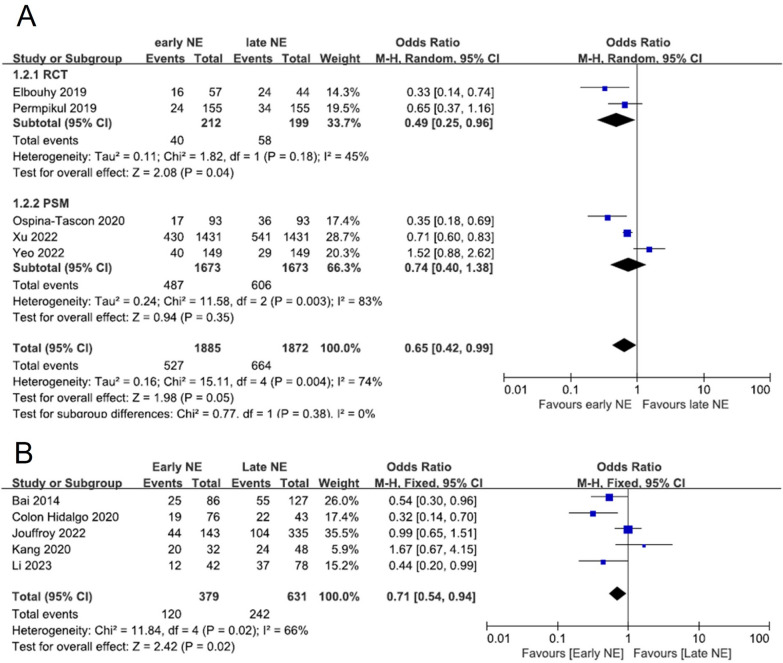
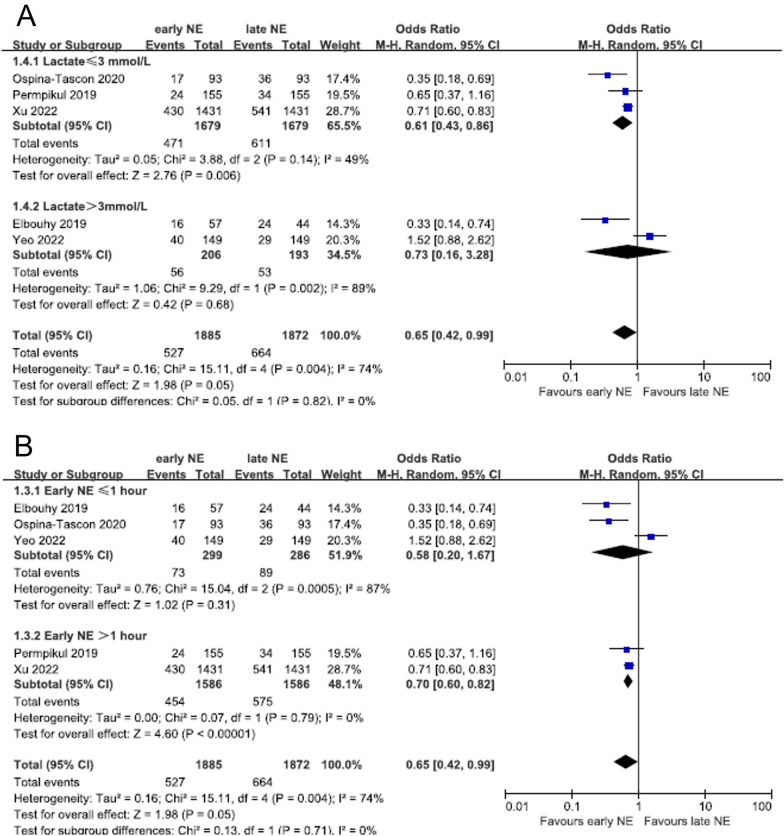
Results: Ten studies (two RCT, three PSM and five observational studies) involving 4767 patients were included. Early norepinephrine significantly reduced mortality in RCT (OR 0.49, 95%CI 0.25-0.96; I2 = 45%, p = 0.04), pooled RCT and PSM (OR 0.65, 95%CI 0.42-0.99; I2 = 74%, p = 0.05), and observational studies (OR 0.71, 95%CI 0.54-0.94; I2 = 66%). The trial sequential analysis indicated more data are needed. Subgroup analyses showed reduced mortality with early norepinephrine when lactate was ≤ 3mmol/L and administered within 1 h. Secondary outcomes showed a reduced fluid volume at 6h (RCT + PSM: mean difference -502 mL, 95%CI -899 to -106; I2 = 91%, p = 0.01), faster MAP target achievement (RCT + PSM: mean difference -1.30h, 95%CI -1.75 to -0.85; I2 = 0%, p < 0.01), more mechanical ventilation-free days (RCT + PSM: mean difference 3.99 days, 95%CI 2.42-5.57; I2 = 32%, p < 0.01) and smaller cumulative norepinephrine dose (Observational: mean difference -3.44 mcg/kg, 95%CI -6.13 to -0.76; I2 = 0%, p = 0.01) in the early initiation group compare to the non-early initiation group.
Conclusion: Early norepinephrine introduction in septic shock is associated with reduced mortality, decreased fluid volume administered at 6 h, faster time to achieve MAP target and more mechanical ventilation-free days. However, the trial sequential analysis indicates that further RCT are still needed to confirm these findings.
Keywords: Acute circulatory failure; Fluids; Hemodynamic; Timing; Vasopressor.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Human ethics and consent to participate declarations: Not applicable. Competing interests: X.M. is a member of the Medical Advisory Board of Pulsion Medical Systems (Getinge) and received honoraria for lectures from Pulsion Medical Systems (Getinge), Baxter and AOP health. The authors declare no competing interests.
Figures


References
-
- Persichini R, Silva S, Teboul J-L, Jozwiak M, Chemla D, Richard C, et al. Effects of norepinephrine on mean systemic pressure and venous return in human septic shock. Crit Care Med. 2012;40:3146–53. - PubMed
-
- Ospina-Tascón GA, Aldana JL, GarcíaMarín AF, Calderón-Tapia LE, Marulanda A, Escobar EP, et al. Immediate norepinephrine in endotoxic shock: effects on regional and microcirculatory flow. Crit Care Med. 2023;51:e157–68. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
