

Association between visual hallucinations and cognitive performance in Lewy body dementia and Alzheimer's disease: A cross-sectional study
- PMID: 40330106
- PMCID: PMC12053050
- DOI: 10.1177/25424823251339132
Association between visual hallucinations and cognitive performance in Lewy body dementia and Alzheimer's disease: A cross-sectional study
Abstract
Background: Visual hallucinations (VH) are an important neuropsychiatric feature of dementia. The association between VH and cognition remains controversial.
Objective: To investigate the differences in clinical correlates of VH and explore the associations between VH and cognitive functional decline in individuals with dementia with Lewy bodies (DLB) and Alzheimer's disease (AD).
Methods: Outpatient medical records of 154 patients with DLB and 297 patients with AD between January 2017 and December 2023 were reviewed. We collected demographic characteristics and used neuropsychological assessments and semi-structured detailed interviews to evaluate cognition and VH. Multiple linear regression and mediation analyses were employed to analyze the data, adjusting for confounding variables.
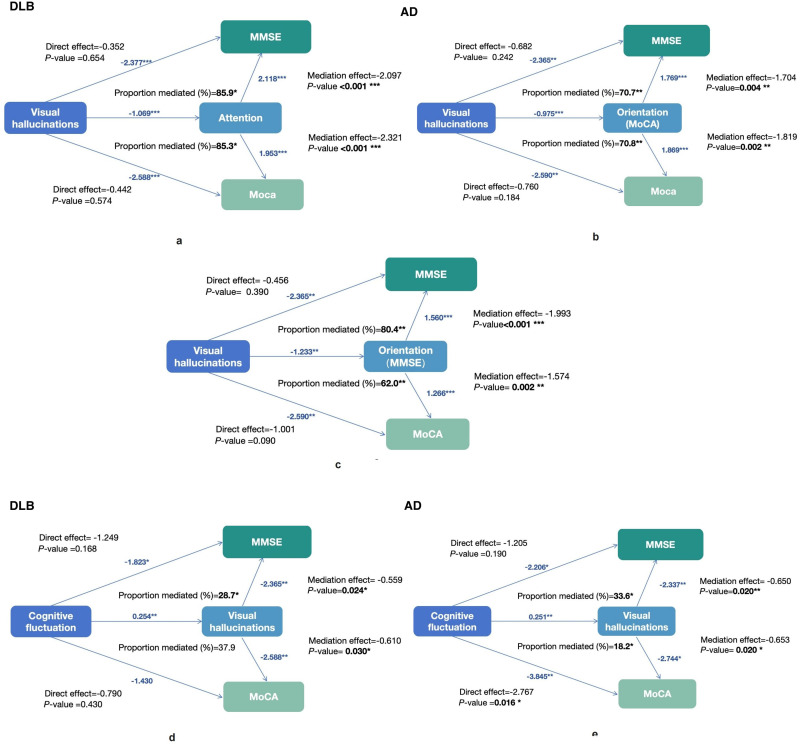
Results: DLB patients had a higher prevalence of VH than AD patients (p < 0.01). The presence of VH predicted lower Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) scores in both DLB and AD patients (p < 0.01). In DLB patients, VH were associated with lower attention function scores after adjustment (p = 0.027). In AD patients, VH were related to worsened orientation ability after adjustment (p = 0.033). Attention function partially mediated the association between VH and cognition in DLB patients (p < 0.01), whereas orientation function partially mediated this association in AD patients (p < 0.01).
Conclusions: VH may independently correlate with deterioration in global cognitive performance. In DLB patients with VH, attentional function appears to be more impaired, whereas in AD patients, orientation function is the most affected. Different cognitive domains may help distinguish between DLB and AD patients with VH.
Keywords: Alzheimer's disease; Lewy bodies; cognitive impairment; dementia; visual hallucinations.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
-
- Tabata K, Saijo Y, Morikawa F, et al. Association of premorbid personality with behavioral and psychological symptoms in dementia with Lewy bodies: comparison with Alzheimer’s disease patients: premorbid personality and BPSD. Psychiatry Clin Neurosci 2017; 71: 409–416. - PubMed
-
- Swann P, O’Brien JT. Management of visual hallucinations in dementia and Parkinson’s disease. Int Psychogeriatr 2019; 31: 815–836. - PubMed
LinkOut - more resources
Full Text Sources
