

Pilot Study: RoboticScope (Robotic Microscope)-assisted Primary Cleft Palate Surgery
- PMID: 40330164
- PMCID: PMC12055182
- DOI: 10.1097/GOX.0000000000006744
Pilot Study: RoboticScope (Robotic Microscope)-assisted Primary Cleft Palate Surgery
Abstract
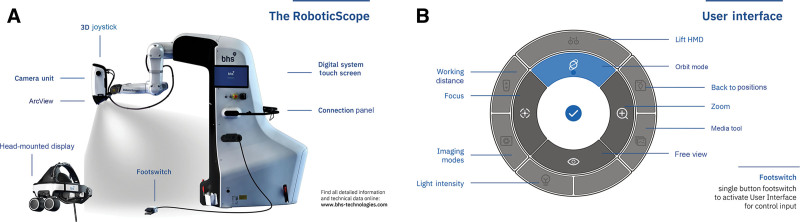
Background: Conventional palatoplasty involves operating in a narrow oral cavity space with surgical loupe visualization. Today, some surgeons resort to surgical microscopes to improve visualization and obtain more precise muscle dissection. The RoboticScope is a head movement-controlled system that moves the robotic arm loaded with 3-dimensional visualization technology, allowing surgeons complete freedom to use their hands during surgery.
Methods: This was a retrospective pilot analysis of 8 pediatric patients, split into 2 cohorts of 4, comparing conventional palatoplasty to RoboticScope-assisted palatoplasty performed in 2023. Patient demographics collected included age, sex, and cleft palate classification (Veau I-IV). Variables measured included operative time, postoperative analgesia, oral intake, hospital stay, and complication rates. Ergonomic evaluations were performed through surgeons documenting their feedback on comfort and surgical efficiency, including dissection and repair.
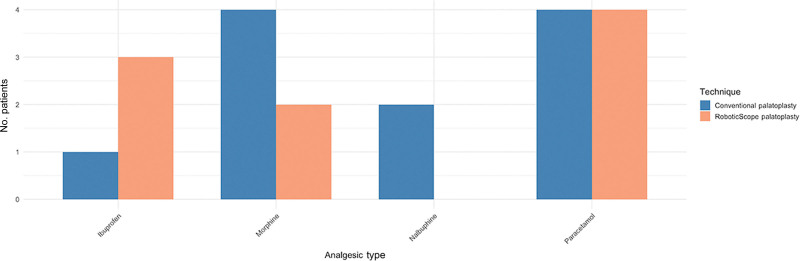
Results: RoboticScope-assisted palatoplasty averaged 28 minutes longer than the conventional method. Postoperative analgesic needs also differed: 100% of the patients who underwent conventional palatoplasty required morphine, whereas only 50% of the RoboticScope patients required morphine. Seventy-five percent of the RoboticScope patients demonstrated good oral intake on day 1, and 50% of the patients were discharged 1 day earlier than the conventional group.
Conclusions: This study concludes that RoboticScope-assisted palatoplasty is safe and feasible, and is associated with fewer analgesic needs, better oral intake, and ergonomic benefits for surgeons than conventional palatoplasty. However, due to the limited nature of the study sample, future multicenter studies with a larger cohort group would be essential to validate these outcomes.
Copyright © 2025 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
The authors have no financial interest to declare in relation to the content of this article. Disclosure statements are at the end of this article, following the correspondence information.
Figures




References
-
- Penny C, McGuire C, Bezuhly M. A systematic review of feeding interventions for infants with cleft palate. Cleft Palate Craniofac J. 2022;59:1527–1536. - PubMed
-
- Bardach J, Salyer KE. Surgical Techniques in Cleft Lip and Palate. Year Book Medical Publishers; 1987.
LinkOut - more resources
Full Text Sources