

Cabrol Procedure in Complex Aortic Root Reconstruction: A Case Series of Three Young Patients With Acute Aortic Syndrome
- PMID: 40330263
- PMCID: PMC12055416
- DOI: 10.1002/ccr3.70452
Cabrol Procedure in Complex Aortic Root Reconstruction: A Case Series of Three Young Patients With Acute Aortic Syndrome
Abstract
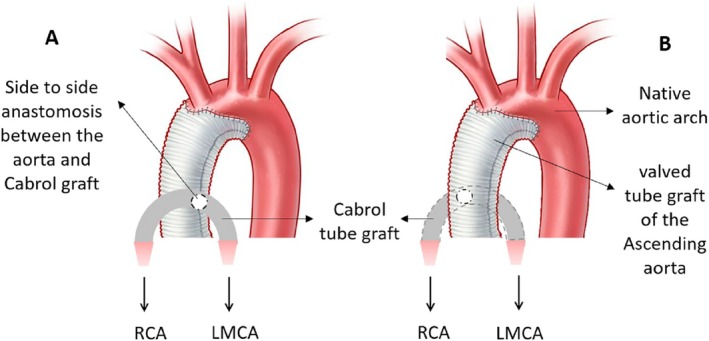
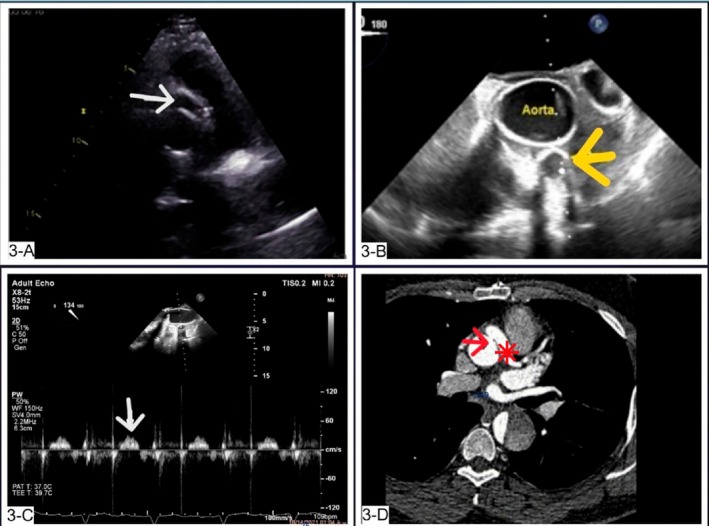
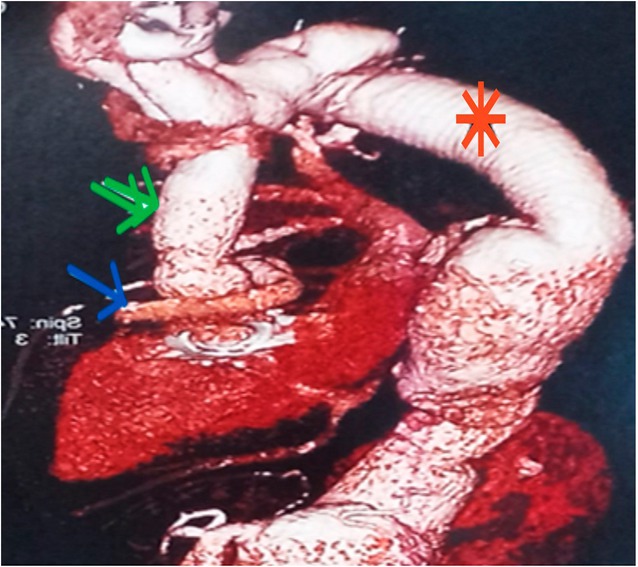
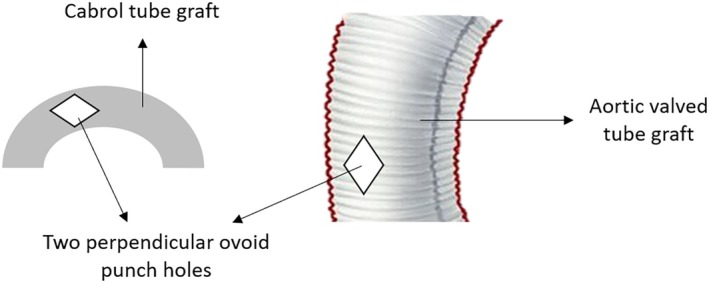
Acute aortic dissection is a rare but life-threatening syndrome, being accompanied by a mortality rate of 1%-2% per hour after the onset of symptoms if they remain untreated. The definitive therapy for type A acute aortic dissection is considered to be emergency surgery. However, the optimal method for aortic root reconstruction has been a controversial issue. This study presents three cases of acute thoracic aortic dissection (TAD) accompanied by complicated aortic root anatomy. These critical conditions were managed successfully with the Cabrol procedure. In this procedure, the coronary ostia are anastomosed to a second graft in an end-to-end fashion, which is then connected side to side with the ascending aorta. A 2-year follow-up of patients showed they had no new signs or symptoms or reemergence of them during this period. Follow-up transthoracic echocardiography (TTE) and computed tomography angiography (CTA) of the aorta showed no evidence of obstruction or complications of Cabrol and aortocoronary anastomosis. Although the modified Bentall procedure using coronary ostial aortic "buttons" may produce superior results and currently represents the standard of care for aortic root reconstruction, the Cabrol procedure can be considered a clinically valuable rescue procedure in patients whose management becomes more complicated due to anatomic difficulties.
Keywords: acute dissection aorta; cardiac surgery; case series; interventional cardiology.
© 2025 The Author(s). Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Myocardial ischemia 10 years after a modified Cabrol procedure in a 42-year-old patient with Marfan syndrome.BMC Cardiovasc Disord. 2020 Oct 27;20(1):461. doi: 10.1186/s12872-020-01740-6. BMC Cardiovasc Disord. 2020. PMID: 33109088 Free PMC article.
-
Evolution and current applications of the Cabrol procedure and its modifications.Ann Thorac Surg. 2011 May;91(5):1636-41. doi: 10.1016/j.athoracsur.2011.01.061. Epub 2011 Mar 27. Ann Thorac Surg. 2011. PMID: 21444065 Review.
-
Early stenosis in a Gore-Tex graft connected to the left main: an emergency transradial angioplasty for a complication in a Cabrol procedure.J Invasive Cardiol. 2012 Oct;24(10):539-42. J Invasive Cardiol. 2012. PMID: 23043039
-
Reoperation for ascending aortic aneurysm, coronary ostial aneurysm and patent Cabrol trick after bentall operation for aortitis syndrome.Circ J. 2005 Jul;69(7):861-4. doi: 10.1253/circj.69.861. Circ J. 2005. PMID: 15988114
-
Complex Bentall Operation: Clinical Pearls to Standardize the Procedure.Ann Thorac Surg. 2025 Apr;119(4):744-754. doi: 10.1016/j.athoracsur.2024.09.013. Epub 2024 Sep 19. Ann Thorac Surg. 2025. PMID: 39306062 Review.
References
-
- Bossone E., LaBounty T. M., and Eagle K. A., “Acute Aortic Syndromes: Diagnosis and Management, an Update,” European Heart Journal 39, no. 9 (2018): 739–749. - PubMed
-
- Isselbacher E. M., Preventza O., J. Hamilton Black, 3rd , et al., “2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines,” Circulation 146, no. 24 (2022): e334–e482. - PMC - PubMed
-
- Sadeghian M., Ebrahimi P., Soltani P., Ghasemi M., Taheri H., and Mehrpooya M., “Successful Management of a Delayed Presentation of Traumatic Descending Thoracic Aorta Pseudoaneurysm: A Literature Review Based on a Case Report,” International Journal of Emergency Medicine 17, no. 1 (2024): 87. - PMC - PubMed
-
- Yamamoto T., Kimura N., Hori D., et al., “Morphological Characteristics and Outcomes of Aortic Repair of Acute Type A Aortic Dissection Occurring in Patients With Aortic Arch Branching Variants,” Surgery Today 55 (2025): 414–424. - PubMed
LinkOut - more resources
Full Text Sources
