

Novel Transungual Approach Using a Cement Spacer for a Recurrent Intramedullary Glomus Tumour of the Finger: A Case Report
- PMID: 40330347
- PMCID: PMC12052036
- DOI: 10.7759/cureus.81764
Novel Transungual Approach Using a Cement Spacer for a Recurrent Intramedullary Glomus Tumour of the Finger: A Case Report
Abstract
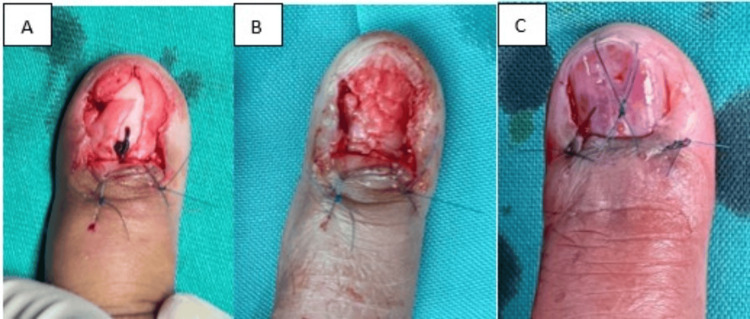
Glomus tumours are rare benign epithelial and mesenchymal neoplasms of the glomus body, which primarily occur in the subungual area of fingers, characterized by excruciating pain, point tenderness, and cold sensitivity. Glomus tumours are also reported to be extradigital in almost every organ, which makes them difficult to diagnose due to their rarity. Delayed diagnosis commonly happens due to negative imaging from plain radiograph and ultrasound imaging. Early recognition of this disease with proper diagnosis and complete surgical excision is typically effective, leading to resolution of symptoms. Despite there is a chance of recurrence even with surgical excision in some cases, probably due to incomplete excision or the presence of another undiagnosed tumour at the beginning. We present a rare case of a recurrent intramedullary glomus tumour of the finger that persisted despite multiple surgical excisions. This case was managed using a novel transungual surgical approach, incorporating a cement spacer to provide structural support for the finger pulp following the removal of the diseased distal phalanx. We also review the surgical outcomes in this challenging scenario.
Keywords: bone cement; excision; glomus tumour; intramedullary; recurrent.
Copyright © 2025, Ooi et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures






References
-
- Reappearance of a glomus tumor of the finger after nine years - a rare case report and literature review. Patel J, Vaish A, Vaishya R, Singhal S. J Orthop Rep. 2022;1:38–41.
-
- Subungual glomus tumors: evaluation with MR imaging. Drapé JL, Idy-Peretti I, Goettmann S, et al. Radiology. 1995;195:507–515. - PubMed
-
- The anatomic location of digital glomus tumor recurrences. Gandhi J, Yang SS, Hurd J. J Hand Surg Am. 2010;35:986–989. - PubMed
Publication types
LinkOut - more resources
Full Text Sources