

From Symptoms to Solution: A Diagnostic Challenge of Whipple's Disease
- PMID: 40330368
- PMCID: PMC12052297
- DOI: 10.7759/cureus.81767
From Symptoms to Solution: A Diagnostic Challenge of Whipple's Disease
Abstract
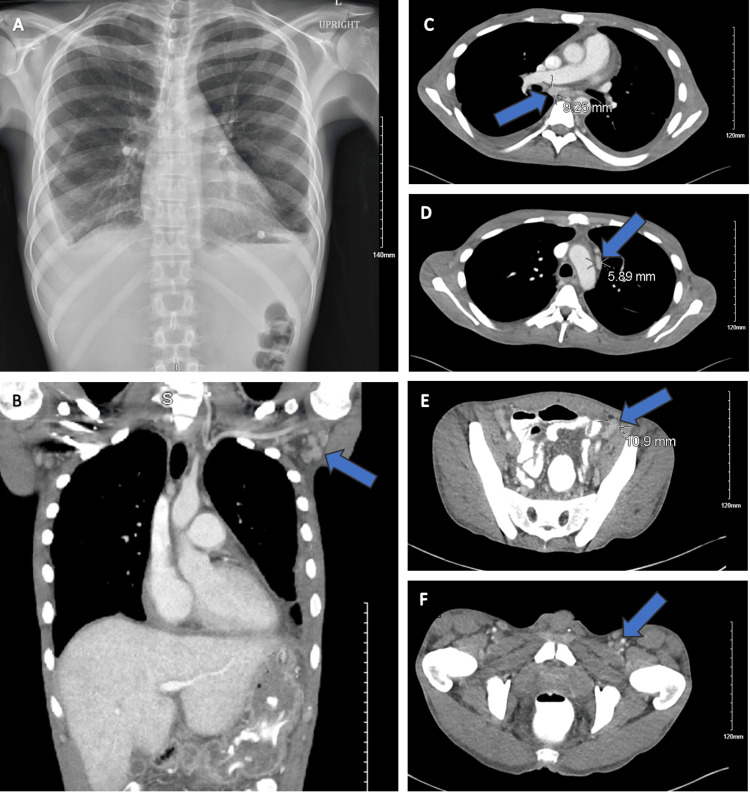
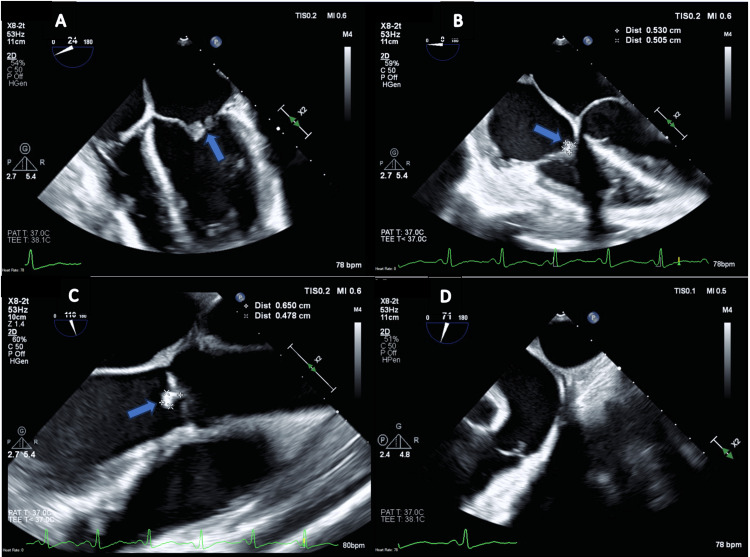
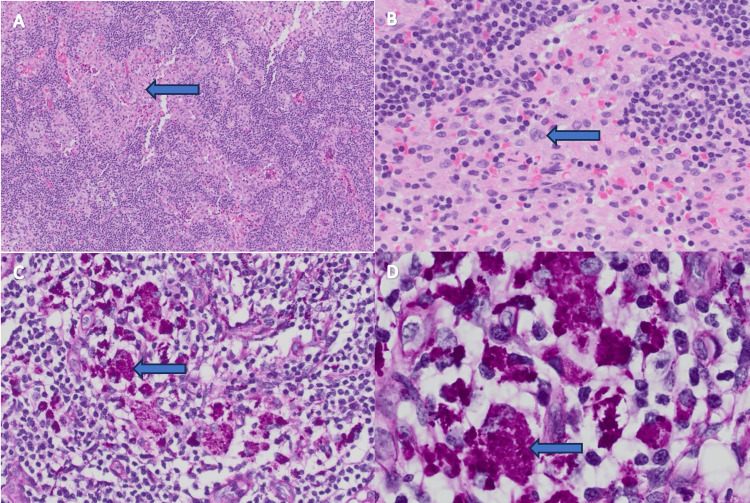
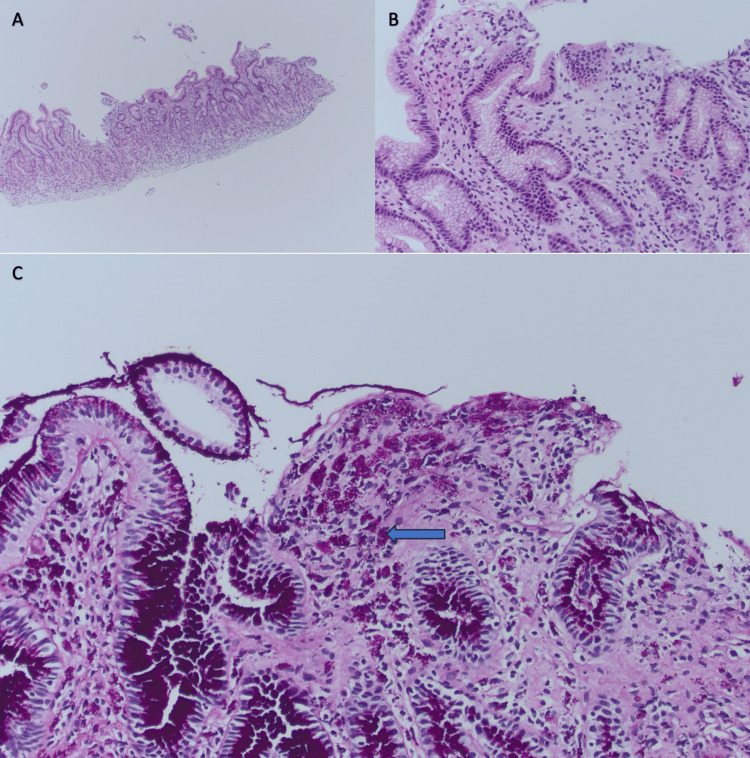
Whipple's disease is caused by the bacterium Tropheryma whipplei. The classic presentation of this disease consists of arthralgias, weight loss, diarrhea, and abdominal pain. However, Whipple's disease can also have other manifestations across multiple organ systems, ranging from lymphadenopathy to pleuropulmonary disease to endocarditis to skin hyperpigmentation and even CNS involvement. We present the case of a 39-year-old male with multiple organ system manifestations of Whipple's disease. He presented with a 50-pound unintentional weight loss, early satiety, arthralgias, chronic cough, pleural effusions, and lymphadenopathy on a CT scan. A transesophageal echocardiogram revealed vegetation on multiple valves, consistent with the diagnosis of endocarditis. Blood cultures showed no growth. Several labs were obtained for a complete work-up for culture-negative endocarditis. The serum polymerase chain reaction (PCR) was reported positive for T. whipplei. Gastric antral biopsy and inguinal lymph node biopsy showed periodic acid-Schiff (PAS)-positive macrophages, confirming the diagnosis of Whipple's disease. The patient was treated with ceftriaxone for a four-week course, followed by Bactrim DS for one year. As was the case with this patient, Whipple's disease can present a wide array of symptoms across multiple organ systems. It is often difficult to diagnose due to its rarity and broad range of non-specific symptoms. Physicians should maintain a high level of suspicion for this disease and include it in their differential diagnosis. A prompt diagnosis and appropriate treatment will yield better outcomes.
Keywords: arthralgias; culture negative infective endocarditis; lymphadenopathy; malabsorption syndrome; tropheryma whipplei; whipple's disease.
Copyright © 2025, Rutherford et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Whipple's disease presenting as weight gain and constipation in a Chinese woman.BMC Infect Dis. 2023 May 8;23(1):302. doi: 10.1186/s12879-023-08276-y. BMC Infect Dis. 2023. PMID: 37158848 Free PMC article.
-
Whipple's in the valleys: a case of Whipple's with thrombocytopenia and endocarditis.J Clin Pathol. 2014 May;67(5):445-8. doi: 10.1136/jclinpath-2013-201915. Epub 2014 Jan 23. J Clin Pathol. 2014. PMID: 24459171
-
A Case Report of Whipple's Disease: A Challenging Diagnosis.Cureus. 2023 Jun 27;15(6):e41021. doi: 10.7759/cureus.41021. eCollection 2023 Jun. Cureus. 2023. PMID: 37519601 Free PMC article.
-
Another Whipple's triad? Pericardial, myocardial and valvular disease in an unusual case presentation from a Canadian perspective.BMC Cardiovasc Disord. 2019 Dec 23;19(1):312. doi: 10.1186/s12872-019-1257-2. BMC Cardiovasc Disord. 2019. PMID: 31870305 Free PMC article. Review.
-
Short article: Relapsing Whipple's disease: a case report and literature review.Eur J Gastroenterol Hepatol. 2016 Mar;28(3):267-70. doi: 10.1097/MEG.0000000000000539. Eur J Gastroenterol Hepatol. 2016. PMID: 26649803 Review.
References
-
- Whipple's disease: a rare disease that can be spotted by many doctors. Cappellini A, Minerba P, Maimaris S, Biagi F. Eur J Intern Med. 2024;121:25–29. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials