

Analgesic Efficacy of Ultrasound-Guided Erector Spinae Plane Block in Patients with Extrahepatic Portal Venous Obstruction Undergoing Splenectomy: A Randomized Controlled Trial
- PMID: 40330384
- PMCID: PMC12051695
- DOI: 10.7759/cureus.81758
Analgesic Efficacy of Ultrasound-Guided Erector Spinae Plane Block in Patients with Extrahepatic Portal Venous Obstruction Undergoing Splenectomy: A Randomized Controlled Trial
Abstract
Background: Postoperative pain is quite prevalent in patients undergoing splenectomy and shunt surgery for extrahepatic portal venous obstruction (EHPVO) via midline laparotomy incision. Most of these patients present with thrombocytopenia in the preoperative period. The presence of thrombocytopenia excludes the placement of epidural catheter for postoperative analgesia, which is considered the gold standard for laparotomies. Systemic opioids remain the cornerstone of pain management in such cases, but they have their side effects. Better alternatives need to be explored to improve postoperative pain management and recovery. The erector spinae plane block (ESPB) has an excellent risk-benefit ratio and has been used for a wide range of cases, from acute postoperative pain to chronic pain conditions.
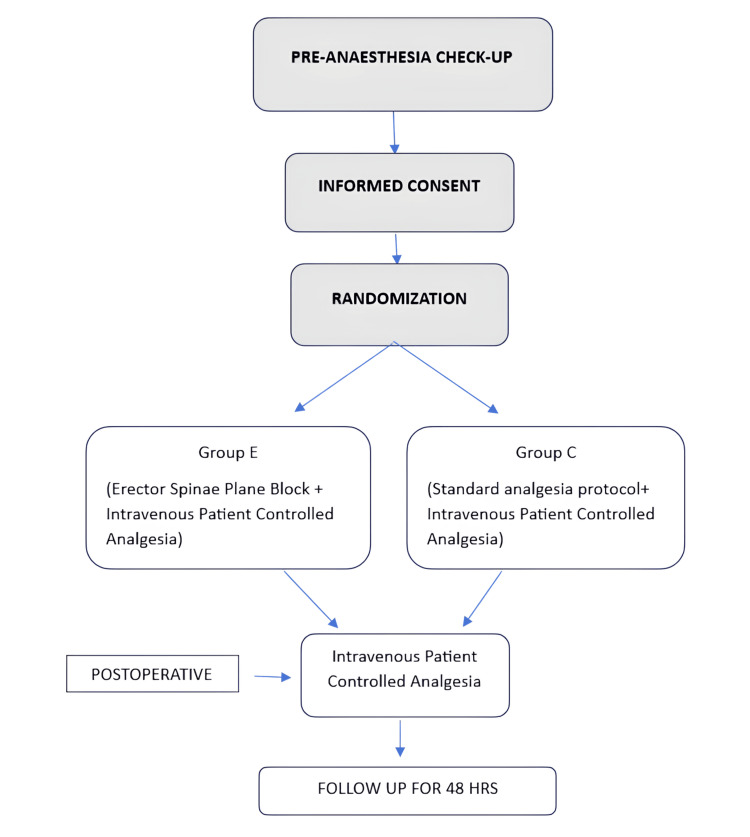
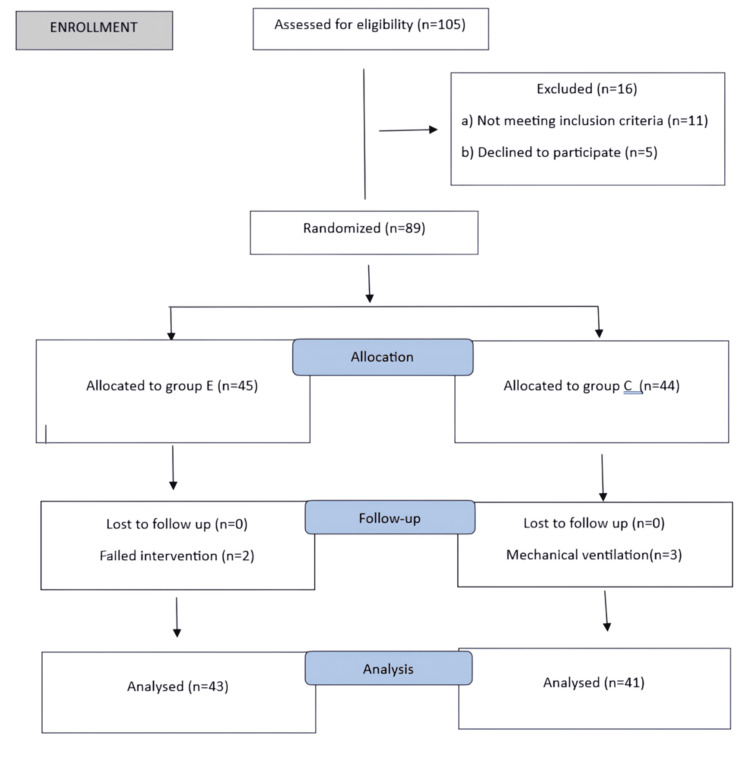
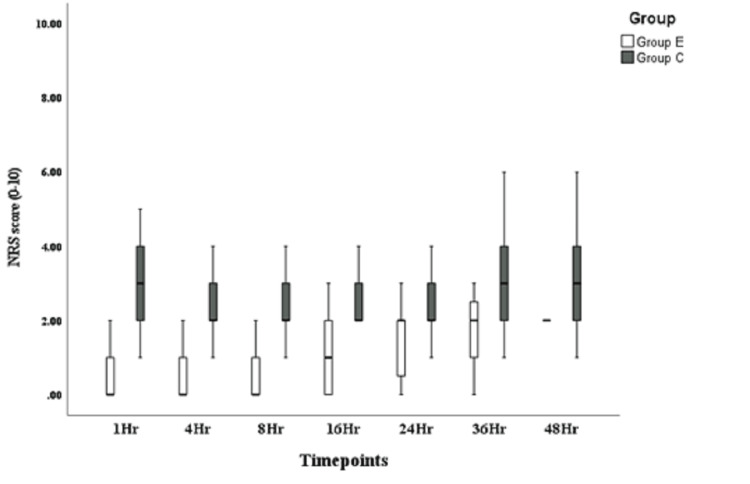
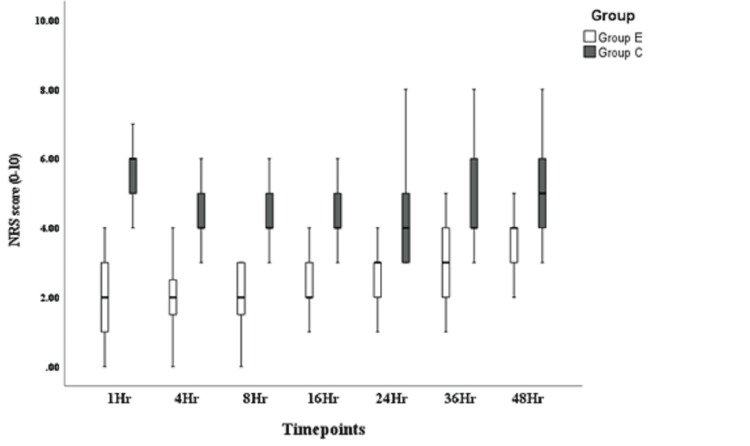
Methodology: This was a randomized controlled trial conducted on 84 patients who underwent splenectomy with lienorenal shunt surgery under general anesthesia. Patients in the study group were given ESPB before extubation, while the control group was managed on conventional analgesics. The primary objective was postoperative opioid requirement by intravenous patient-controlled analgesia (PCA) in both groups. Secondary objectives were static and dynamic Numerical Rating Scale (NRS) scores, hospital stay duration, time first to rescue analgesia, and incidences of adverse events.
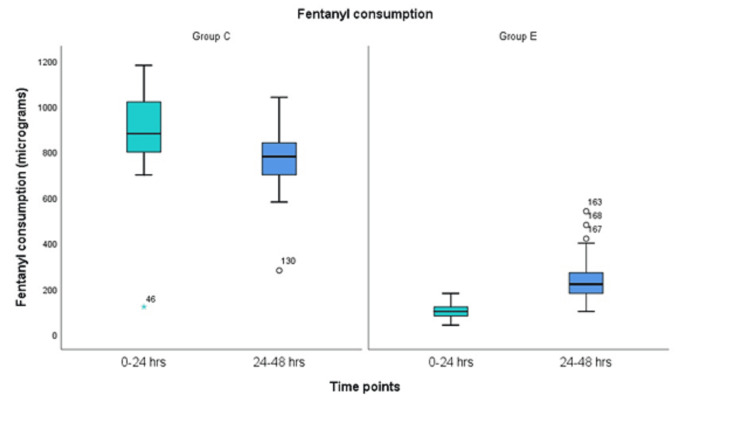
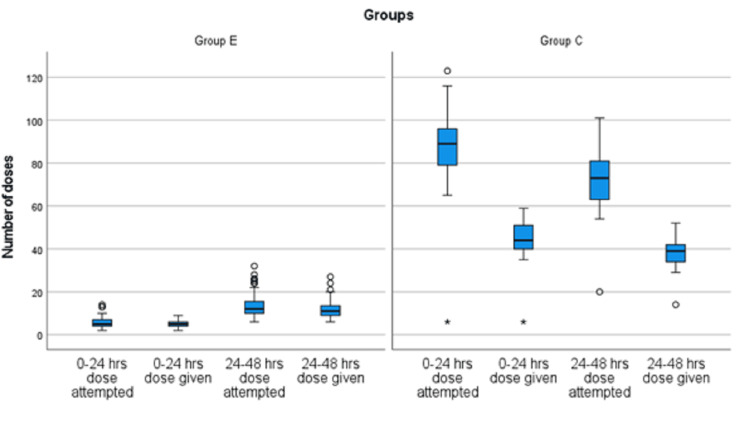
Results: Patients in the ESPB group had less requirement of fentanyl in the postoperative period (median of 100 µg as compared to 880 µg in control group in first 24 hours). Static and dynamic pain scores were also less in the ESPB group at all time points (P < 0.001). Adverse events were higher in the control group compared to the ESPB group.
Conclusions: Ultrasound-guided ESPB provides superior analgesia and recovery with fewer side effects than conventional analgesics.
Keywords: analgesia; epidural analgesia; erector spinae plane block; paravertebral block; splenectomy; thrombocytopenia.
Copyright © 2025, Ambasta et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institute Ethics Committee, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow issued approval 2021-57-IP-119. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Ultrasound-Guided Techniques for Postoperative Analgesia in Patients Undergoing Laparoscopic Sleeve Gastrectomy: Erector Spinae Plane Block vs. Quadratus Lumborum Block.Pain Physician. 2023 May;26(3):245-256. Pain Physician. 2023. PMID: 37192227 Clinical Trial.
-
Efficacy of ultrasound-guided erector spinae plane block on analgesia and quality of recovery after minimally invasive direct coronary artery bypass surgery: protocol for a randomized controlled trial.Trials. 2024 Jan 19;25(1):65. doi: 10.1186/s13063-024-07925-0. Trials. 2024. PMID: 38243276 Free PMC article.
-
Ultrasound-guided erector spinae plane block for postoperative analgesia in pediatric patients undergoing splenectomy: A prospective randomized controlled trial.Paediatr Anaesth. 2019 Dec;29(12):1201-1207. doi: 10.1111/pan.13758. Epub 2019 Nov 8. Paediatr Anaesth. 2019. PMID: 31630465 Clinical Trial.
-
Analgesic efficacy and safety of erector spinae plane block in pediatric patients undergoing elective surgery: A systematic review and Meta-analysis of randomized controlled trials.J Clin Anesth. 2024 Nov;98:111575. doi: 10.1016/j.jclinane.2024.111575. Epub 2024 Aug 10. J Clin Anesth. 2024. PMID: 39128258
-
Ultrasound-guided erector spinae plane block for postoperative short-term outcomes in lumbar spine surgery: A meta-analysis and systematic review.Medicine (Baltimore). 2023 Feb 17;102(7):e32981. doi: 10.1097/MD.0000000000032981. Medicine (Baltimore). 2023. PMID: 36800574 Free PMC article.
References
-
- Consensus on extra-hepatic portal vein obstruction. Sarin SK, Sollano JD, Chawla YK, et al. Liver Int. 2006;26:512–519. - PubMed
-
- Etiological spectrum of esophageal varices due to portal hypertension in Indian children: is it different from the West? Poddar U, Thapa BR, Rao KL, Singh K. J Gastroenterol Hepatol. 2008;23:1354–1357. - PubMed
-
- Primary prophylaxis of variceal bleeding in children and the role of Meso-Rex bypass: summary of the Baveno VI pediatric satellite symposium. Shneider BL, de Ville de Goyet J, Leung DH, et al. Hepatology. 2016;63:1368–1380. - PubMed
-
- The effects of three different analgesia techniques on long-term postthoracotomy pain. Sentürk M, Ozcan PE, Talu GK, et al. Anesth Analg. 2002;94:11-5, table of contents. - PubMed
LinkOut - more resources
Full Text Sources