

Dynamics of Multisystem Inflammatory Syndrome in Children (MIS-C) associated to COVID-19: steady severity despite declining cases and new SARS-CoV-2 variants-a single-center cohort study
- PMID: 40332604
- PMCID: PMC12058826
- DOI: 10.1007/s00431-025-06153-1
Dynamics of Multisystem Inflammatory Syndrome in Children (MIS-C) associated to COVID-19: steady severity despite declining cases and new SARS-CoV-2 variants-a single-center cohort study
Abstract
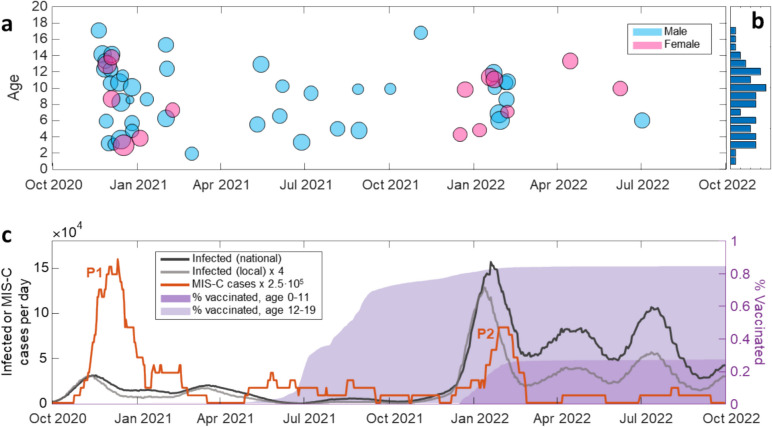
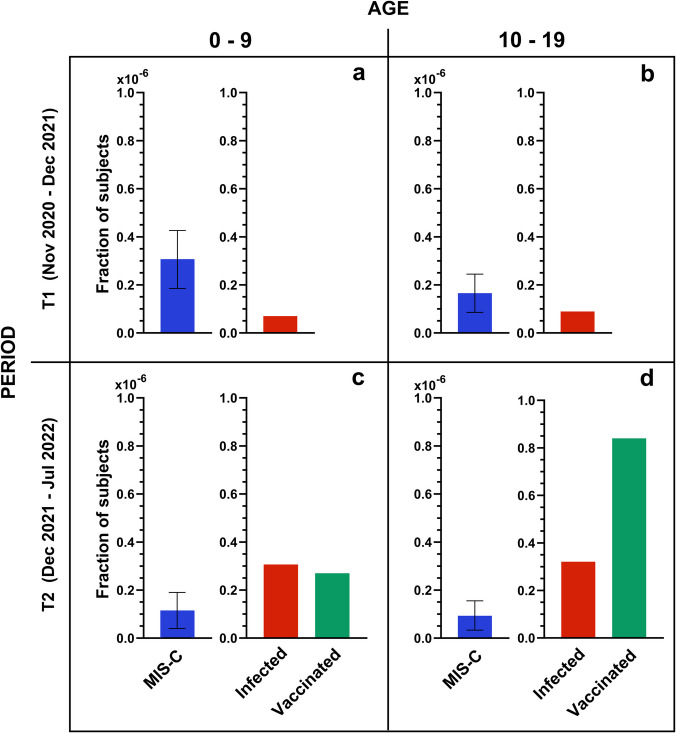
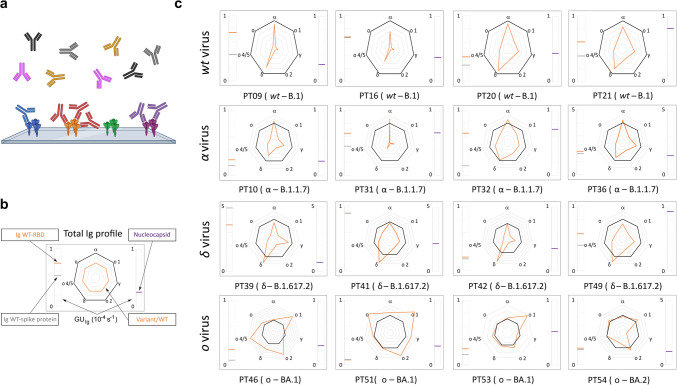
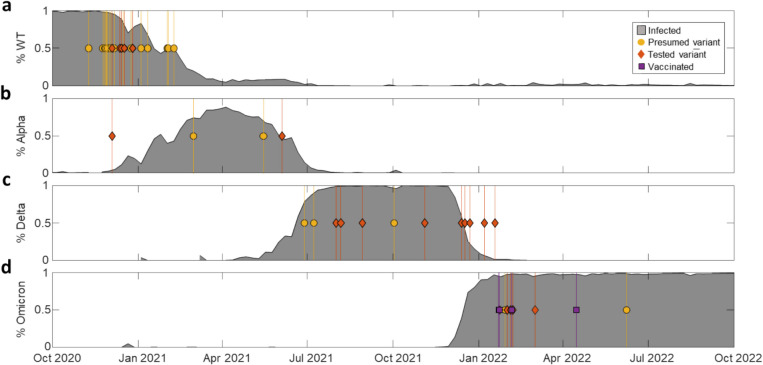
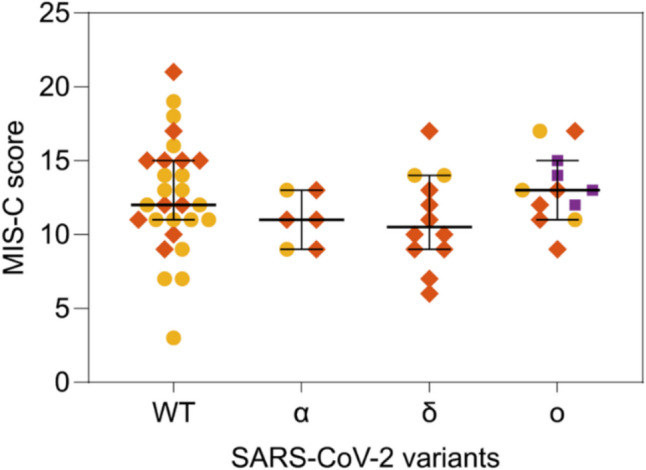
Multisystem Inflammatory Syndrome in Children (MIS-C) is a serious condition associated with SARS-CoV-2 infection. The relationship between SARS-CoV-2 variants of concern (VOCs) and the occurrence and severity of MIS-C is unknown. We analyzed the dynamics of MIS-C in the Milan metropolitan area (Italy) during the COVID-19 pandemic, focusing on the epidemiologic trends and disease severity in relation to different VOCs in a single-center study. Fifty-seven MIS-C patients (mean 8.3 ± 3.8 years) admitted to the Pediatric Department of Buzzi Children's Hospital in Milan, Italy, between November 2020 and July 2022, were retrospectively included in the study. The SARS-CoV-2 variant was retrospectively identified from serological fingerprinting (profiles of serum antibodies targeting different variants of SARS-CoV-2 obtained by a label-free microarray biosensor) or by the variant of prevalence. Two main periods of MIS-C case accumulation were observed. The peak of MIS-C cases rate in December 2020 reached 0.6 cases per day, which is nearly double the rate observed in February 2022, despite the larger number of infected subjects. Although the WT variant exhibited a broader range of severity score values, the score distributions for the different variants do not show statistically relevant differences.
Conclusion: The results clearly show a decrease in the incidence of MIS-C in relation to infections, but also support the concept that severity of MIS-C remained essentially unchanged across different virus variants, including Omicron. The course of MIS-C, once initiated, is independent from the characteristics of the triggering variants, although later variants may be considered less likely to induce MIS-C.
What is known: • MIS-C is a rare systemic inflammatory disorder that arises as a post-infectious complication temporally related to SARS-CoV-2 infection. • Fluctuations in MIS-C incidence were observed throughout the pandemic, with the latest variants associated with a lower incidence.
What is new: • The SARS-CoV-2 variant of infection can be retrospectively confirmed by serum antibody fingerprinting using a label-free microarray biosensor. • Despite the decreasing incidence, MIS-C severity has remained essentially unchanged across SARS-CoV-2 variants.
Keywords: Children; Infection; Label-free microarray biosensor; Multisystem inflammatory syndrome; SARS-CoV-2; Serum antibody fingerprint; Variants of concern.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: The Ethics Committee Milano Area 1 (protocol number 0037072) granted approval for the study. The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board Territorial Area 1_Milano (Protocol number n. MI-1, n. 0034170; protocol number 2021/ST/138). Consent to participate: Informed consent was obtained from all parents and/or guardians involved in the study. Competing interests: The authors declare no competing interests.
Figures
References
-
- Davies P, Evans C, Kanthimathinathan HK, et al. (2020) Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: a multicentre observational study. Lancet Child Adolesc Health 4(9):669–677. 10.1016/S2352-4642(20)30215-7 - PMC - PubMed
-
- Giraldo-Alzate C, Tamayo-Múnera C, López-Barón E, Caicedo-Baez MC, Piñeres-Olave BE (2022) Síndrome inflamatorio multisistémico en niños asociado a COVID-19. Revisión narrativa de la literatura a propósito de un caso. Acta Colombiana de Cuidado Intensivo 22(2):137–148. 10.1016/j.acci.2020.11.002
-
- Haslak F, Gunalp A, Kasapcopur O (2023) A cursed goodbye kiss from severe acute respiratory syndrome-coronavirus-2 to its pediatric hosts: multisystem inflammatory syndrome in children. Curr Opin Rheumatol 35(1):6–16. 10.1097/BOR.0000000000000910 - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
