

Delirium in critically ill children: a retrospective pre- and post-cohort study on the introduction of delirium screening in a paediatric intensive care unit
- PMID: 40332724
- PMCID: PMC12125132
- DOI: 10.1007/s11096-025-01887-2
Delirium in critically ill children: a retrospective pre- and post-cohort study on the introduction of delirium screening in a paediatric intensive care unit
Abstract
Background: Paediatric delirium is a neuropsychiatric disorder with disrupted cerebral functioning due to underlying disease and/or critical care treatment. It has been reported in up to one third of paediatric intensive care admissions, with hypoactive delirium most prevalent in children.
Aim: The aim of this study was to assess whether the introduction of delirium screening was associated with a change in the pharmacotherapy exposure and clinical outcomes.
Method: A retrospective pre and post cohort study of all admissions > 48 h who required mechanical ventilation between 11th March 2019 and 11th March 2021. Cohort 1 (11th March 2019-11th March 2020) prior to the introduction of delirium screening and cohort 2 (12th March 2020-12th March 2021) after delirium screening. Patients < 3 months old, who were never mechanically ventilated, admitted <48 h, continuously receiving neuromuscular blockade or deeply sedated were not included. A multivariate model was created to compare pharmacotherapy use before and after implementation of delirium screening.
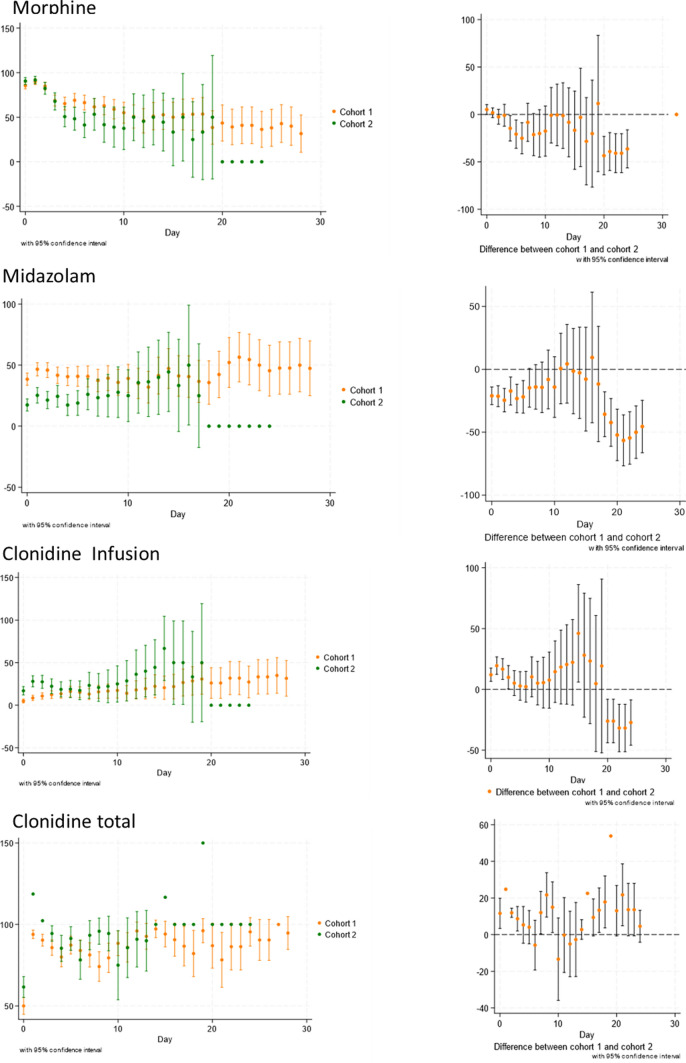
Results: Two thousand and thirty-four patient encounters were identified with 588 meeting the inclusion criteria (364 cohort 1 and 224 cohort 2). There was a reduction in usage of infusions of morphine (decrease in doses of 18% p < 0.05) and midazolam (50% reduction in patients receiving p < 0.05), after screening commenced. Chloral hydrate use was unchanged however cohort 2 received lower daily doses (p < 0.05). Clonidine infusion use increased for cohort 2 (16% v 28% p < 0.05), with lower daily doses (23 v 13 µg/kg/day p < 0.05). Positive clinical outcomes such as decreased duration of mechanical ventilation, length of stay and out of range sedation and withdrawal scores were also observed.
Conclusion: Introduction of a paediatric delirium care bundle including screening tool and associated education was associated with decrease in exposure to modifiable pharmacotherapy risk factors for the development of paediatric delirium. These findings should be further evaluated in future interventional studies.
Keywords: Analgesia and sedation; Paediatric critical care; Paediatric delirium; Pharmacotherapy.
© 2025. The Author(s).
Conflict of interest statement
Conflicts of interest: None.
Figures
References
-
- American Psychiatric Association: Diagnostic and statistical manual of mental disorders: DSM-5. Arlington, VA: American Psychiatric Association; 2013.
-
- Semple D, Howlett MM, Strawbridge JD, et al. A systematic review and pooled prevalence of delirium in critically ill children. Crit Care Med. 2022;50(2):317–28. 10.1097/ccm.0000000000005260. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
