

Assessing the efficacy and safety of different nonsteroidal anti-inflammatory drugs in the treatment of osteoarthritis: A systematic review and network meta-analysis based on RCT trials
- PMID: 40333622
- PMCID: PMC12057957
- DOI: 10.1371/journal.pone.0320379
Assessing the efficacy and safety of different nonsteroidal anti-inflammatory drugs in the treatment of osteoarthritis: A systematic review and network meta-analysis based on RCT trials
Abstract
Introduction: Osteoarthritis (OA) as a degenerative disease, has seen a continuous rise in incidence and prevalence globally since 1990, imposing a significant disease burden. NSAIDs (Nonsteroidal anti-inflammatory drugs) as symptomatic medications for OA treatment, hold an indispensable position in clinical practice.
Objective: To evaluate the efficacy and safety of different NSAIDs in the treatment of OA through Bayesian Network Meta-Analysis (NMA).
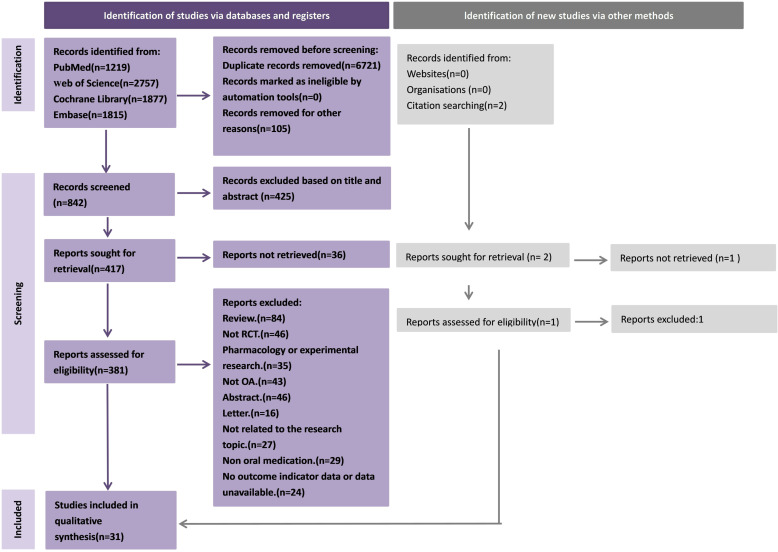
Methods: Randomized controlled trials (RCTs) on NSAIDs for OA treatment were retrieved from PubMed, Web of Science, Embase, and the Cochrane Library databases. The search timeframe was from the inception of each database up to June 1, 2024. Outcome indicators for NMA were all conducted using a random-effects model. MetaInsight and Stata 14.0 software were used in R for calculations and plotting of NMA. Measurement data were represented by mean difference (MD), and count data by odds ratio (OR); a 95% confidence interval (CI) was also calculated for each effect size.
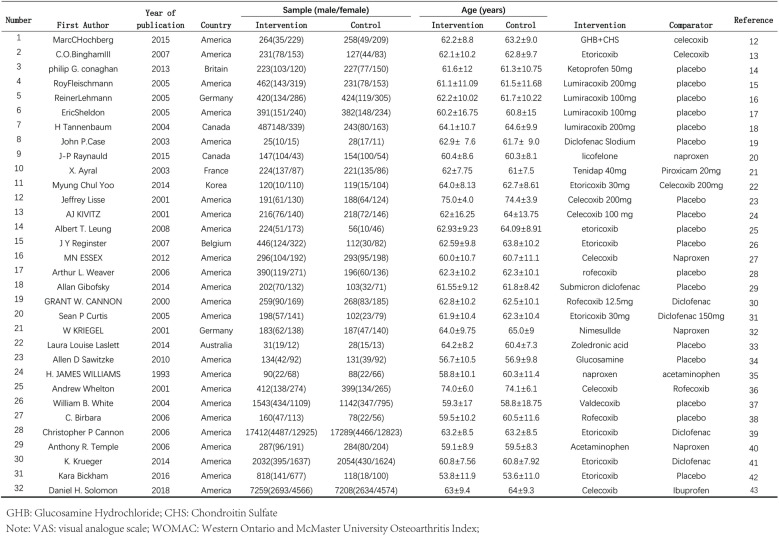
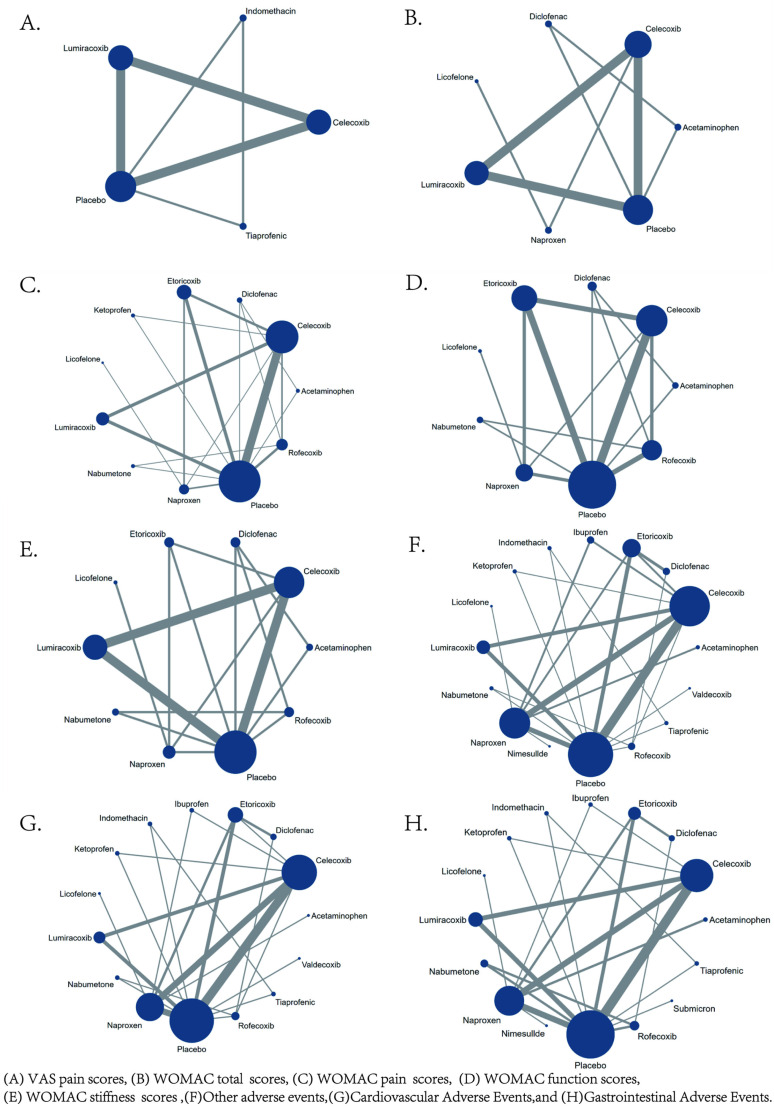
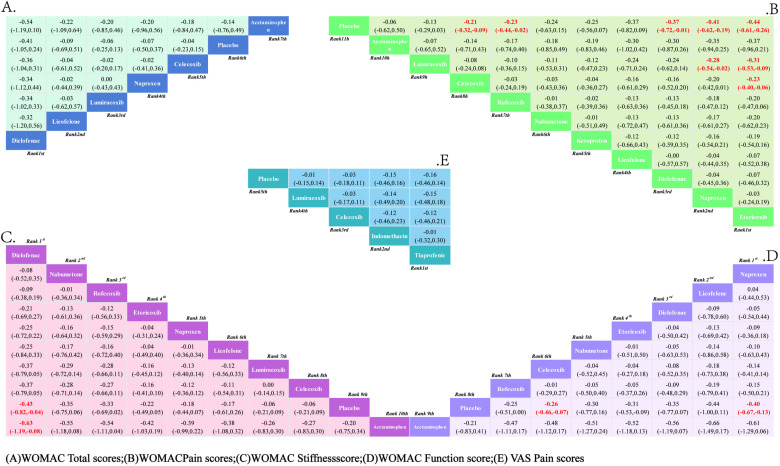
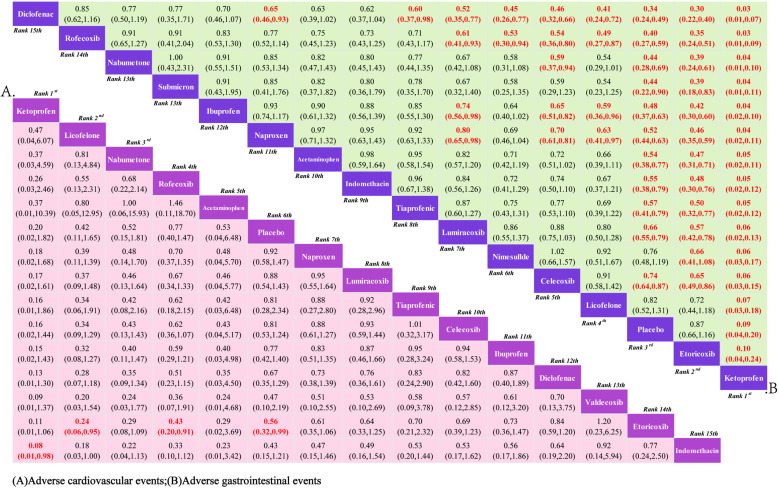
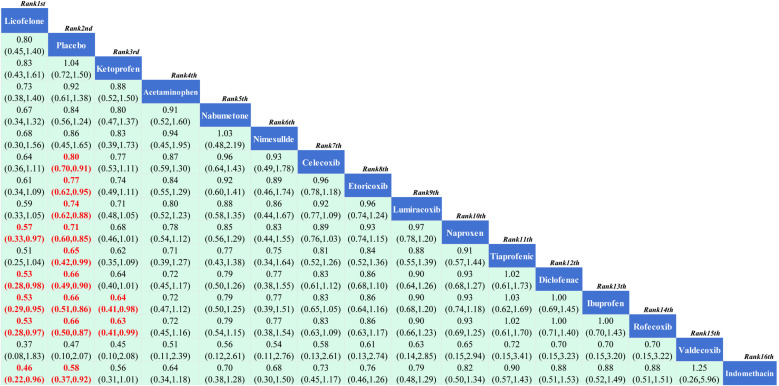
Results: This study included 31 studies, involving 68,539 patients with knee osteoarthritis (KOA) and 16 interventions. NMA results showed that compared to the placebo, Tiaprofenic reduced the VAS score (MD = -0.16, 95% CI: (-0.46 to 0.14), P > 0.05), albeit without significant difference; meanwhile, Diclofenac reduced the total WOMAC score in KOA patients (MD = -0.41, 95% CI: -1.05 to 0.24, P > 0.05). Compared to the placebo, Etoricoxib was the best medication for improving the WOMAC pain subscale score (MD = -0.44; 95% CI: -0.61 to -0.26); Naproxen significantly improved the WOMAC Function score in KOA patients after administration (MD = -0.43; 95% CI: -0.82 to -0.04); Diclofenac intervention significantly reduced the WOMAC Stiffness score in KOA patients (MD = -0.40; 95% CI: -0.67 to -0.13). In terms of adverse event rates, compared to the placebo, the use of Etoricoxib significantly increased the incidence of cardiovascular adverse events (OR = 0.56, 95% CI: 0.32-0.99); Ketoprofen had fewer gastrointestinal adverse events during the medication process (OR = 0.09, 95% CI: 0.04-0.20); Licofelone had a lower rate of other adverse events during the medication process (OR = 0.80, 95% CI: 0.45-1.40, P > 0.05). Therefore, the results indicate that Etoricoxib, Tiaprofenic, Naproxen, Diclofenac, and Ketoprofen have better clinical efficacy and safety.
Conclusion: Compared to other NSAIDs, Etoricoxib, Tiaprofenic, Naproxen, and Diclofenac play a more effective role in improving clinical symptoms of OA; in terms of reducing the incidence of adverse events, Ketoprofen has a lower chance of adverse events. However, the possibility of these results still needs further clinical and basic research for verification.
Copyright: © 2025 JiaoYi et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Geszke-Moritz M, Nowak G, Moritz M, Feist B, Nycz JE. Role of plant materials with anti-inflammatory effects in phytotherapy of osteoarthritis. Curr Top Med Chem. 2025;25(1):35–46. - PubMed
-
- Bodden J, Joseph GB, Schirò S, Lynch JA, Lane NE, McCulloch CE, et al.. Opioid users show worse baseline knee osteoarthritis and faster progression of degenerative changes: a retrospective case-control study based on data from the Osteoarthritis Initiative (OAI). Arthritis Res Ther. 2021;23(1):146. doi: 10.1186/s13075-021-02524-9 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
