

Dynamics of care and sector use between birth, contraception and sick child services
- PMID: 40333655
- PMCID: PMC12057983
- DOI: 10.1371/journal.pgph.0004418
Dynamics of care and sector use between birth, contraception and sick child services
Abstract
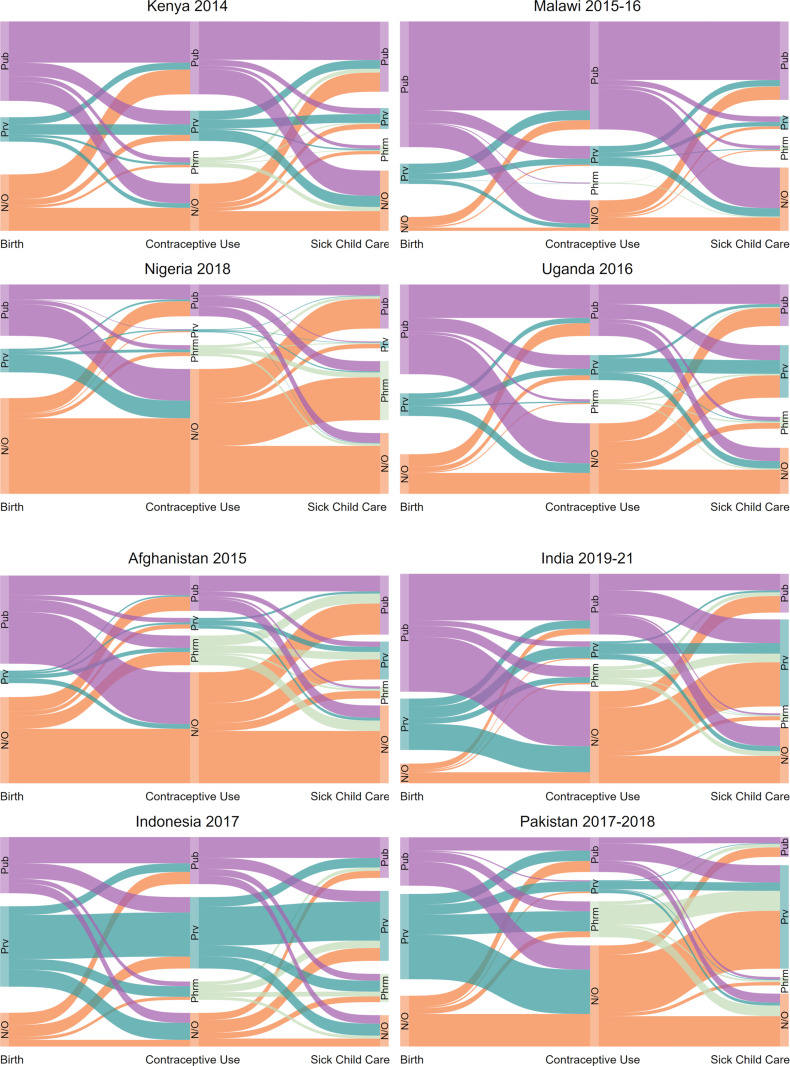
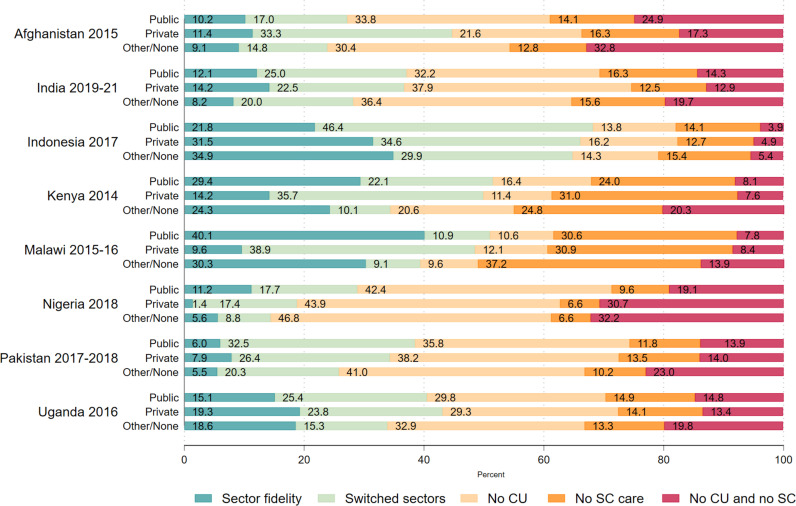
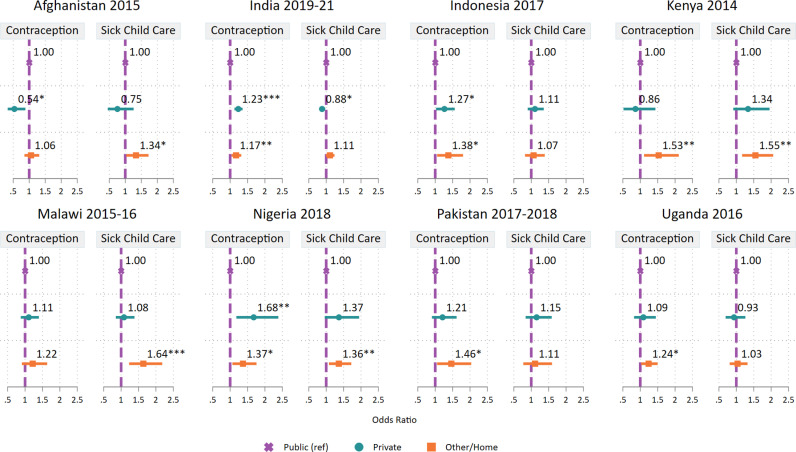
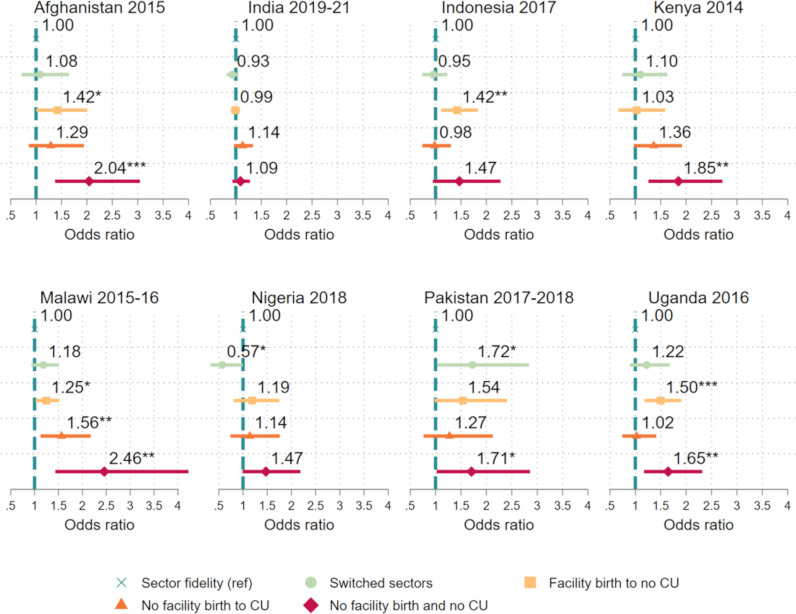
Governments in low- and middle-income countries increasingly recognize their role as stewards of mixed health systems comprising both public and private actors, but policy often lacks a nuanced understanding of how individuals switch between these two sectors for their healthcare needs, especially for family planning (FP) and maternal, newborn and child health (MNCH). In this cross-sectional study, we used data collected by The Demographic and Health Surveys Program between 2014-2021 from eight countries (Afghanistan, India, Indonesia, Kenya, Malawi, Nigeria, Pakistan, and Uganda) to describe service and sector use among women with a recent birth, a need for FP, and a child under five years old experiencing an illness (N = 53,014). We applied multivariable logistic regressions in each country to test the associations first between sector for birth and missed opportunities for contraceptives or sick child care, and next, between sector use dynamics between birth and contraceptive use (sector fidelity, sector switching, or nonuse of services) and nonuse of sick child care. Sector at facility for birth and sector switching between services was common, but neither were generally associated with missed opportunities for care for sick children. However, private sector use at birth predicted nonuse of contraceptives in four countries, though the directionality varied. Consistently, women who did not access care at birth and contraception had significantly greater odds of missing care for sick children. Notably, in Malawi, the adjusted odds ratio of missed sick child care among those with nonuse of care for birth or contraceptives was 2.5 times that of those with sector fidelity (95% Confidence Interval: 1.43-4.22). These findings underscore the need for health system stewards to closely consider both the public and private sectors in health governance. Greater cross-sectoral cooperation and continuity of care is paramount to improving health outcomes.
Copyright: © 2025 Mallick et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Use of family planning and child health services in the private sector: an equity analysis of 12 DHS surveys.Int J Equity Health. 2018 Apr 24;17(1):50. doi: 10.1186/s12939-018-0763-7. Int J Equity Health. 2018. PMID: 29690902 Free PMC article.
-
Pathways to increased coverage: an analysis of time trends in contraceptive need and use among adolescents and young women in Kenya, Rwanda, Tanzania, and Uganda.Reprod Health. 2017 Oct 17;14(1):130. doi: 10.1186/s12978-017-0393-3. Reprod Health. 2017. PMID: 29041936 Free PMC article.
-
Postpartum family planning integration with maternal, newborn and child health services: a cross-sectional analysis of client flow patterns in India and Kenya.BMJ Open. 2018 Apr 3;8(4):e018580. doi: 10.1136/bmjopen-2017-018580. BMJ Open. 2018. PMID: 29615443 Free PMC article.
-
Private sector engagement in the COVID-19 response: experiences and lessons from the Democratic Republic of Congo, Nigeria, Senegal and Uganda.Global Health. 2022 Jun 15;18(1):60. doi: 10.1186/s12992-022-00853-1. Global Health. 2022. PMID: 35705961 Free PMC article. Review.
-
Contraceptive delivery in the developing world.Br Med Bull. 1993 Jan;49(1):27-39. doi: 10.1093/oxfordjournals.bmb.a072604. Br Med Bull. 1993. PMID: 8324614 Review.
References
LinkOut - more resources
Full Text Sources