

Complicated appendicitis presenting as anterior abdominal wall abscess in a diabetic patient: A case report
- PMID: 40334448
- PMCID: PMC12138566
- DOI: 10.1016/j.ijscr.2025.111390
Complicated appendicitis presenting as anterior abdominal wall abscess in a diabetic patient: A case report
Abstract
Introduction: Acute appendicitis is one of the most common surgical emergencies (8.6 % in men and 6.4 % in women), with varying presentations, including complications such as appendicular abscess. While the typical clinical course involves right lower quadrant pain and fever, rare complications can present with atypical symptoms, particularly in high-risk patients such as those with diabetes.
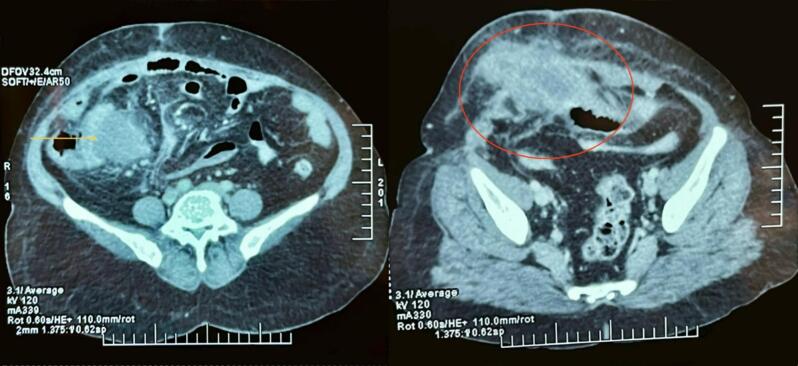
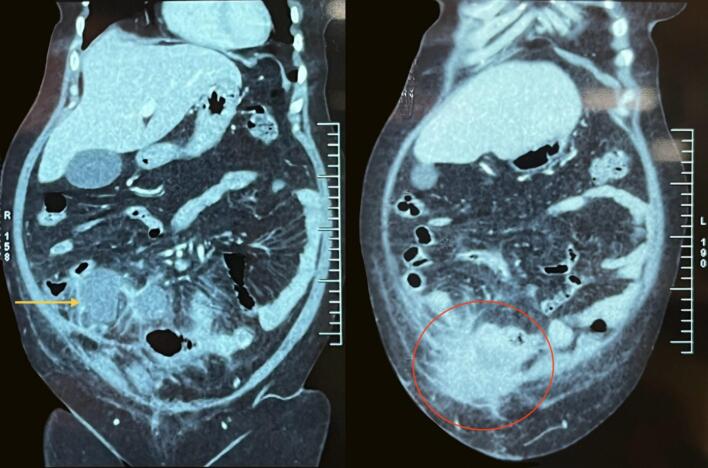
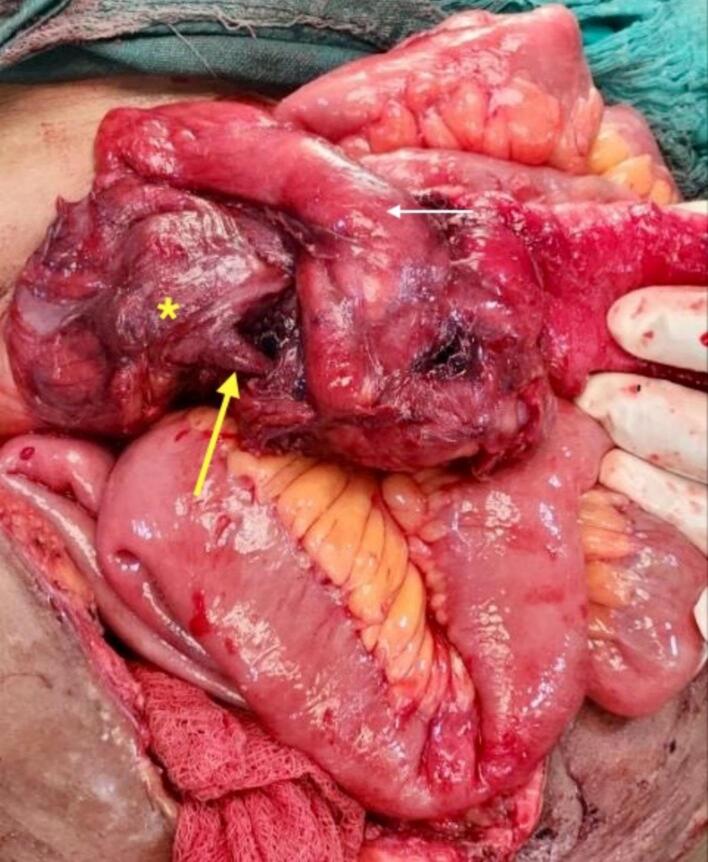
Presentation of case: A 55-year-old diabetic female presented with a 10-day history of worsening abdominal pain, foul-smelling discharge at the anterior abdominal wall below the umbilicus, and fever. Imaging revealed an appendicular abscess extending into the anterior abdominal wall. Emergency exploratory laparotomy showed a perforated appendix with a purulent collection in the peritoneal cavity extending to the anterior abdominal wall, requiring drainage and right hemicolectomy.
Discussion: Perforated appendicitis (incidence of 20-30 %), particularly in diabetic patients, can lead to localized abscesses or soft tissue infections in atypical locations such as the abdominal wall. These rare complications are more likely in immunocompromised individuals, including those with diabetes, where the incidence of perforated appendicitis is notably higher. Early imaging with ultrasonography or Contrast Enhanced Computed Tomography is critical for identifying complicated appendicitis and guiding surgical intervention.
Conclusion: Anterior abdominal wall abscesses as a complication of perforated appendicitis are rare but significant. This case underscores the importance of early and accurate diagnosis, supported by imaging, to guide appropriate surgical management. Timely intervention can help prevent life-threatening conditions such as necrotizing fasciitis, improve patient outcomes, and reduce the risk of postoperative complications, particularly in high-risk populations.
Keywords: Abdominal wall abscess; Case report; Complicated appendicitis; Diabetes; Laparotomy; Perforated appendix.
Copyright © 2025 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Conflict of interest statement The authors have no conflict of interest to declare.
Figures

References
-
- Addiss D.G., Shaffer N., Fowler B.S., Tauxe R.V. The epidemiology of appendicitis and appendectomy in the United States. Am. J. Epidemiol. Nov 1990;132(5):910–925. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
