

Genomic landscape of diffuse glioma revealed by whole genome sequencing
- PMID: 40335506
- PMCID: PMC12059081
- DOI: 10.1038/s41467-025-59156-9
Genomic landscape of diffuse glioma revealed by whole genome sequencing
Abstract
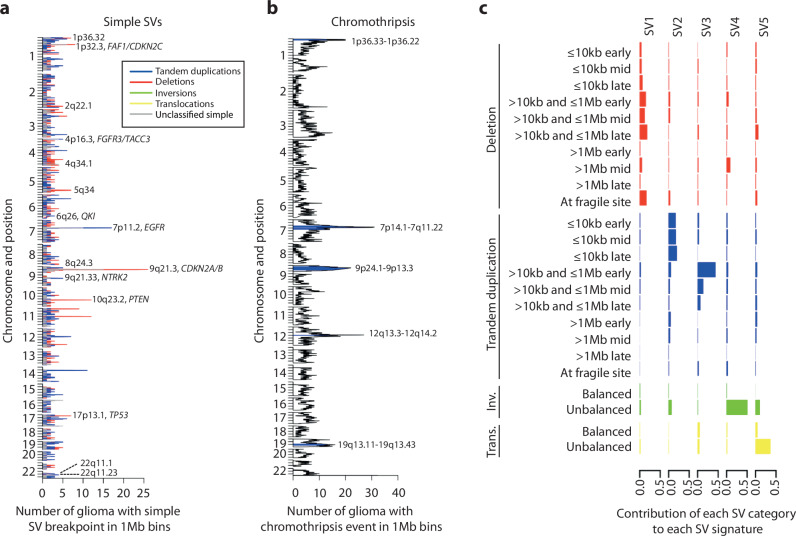
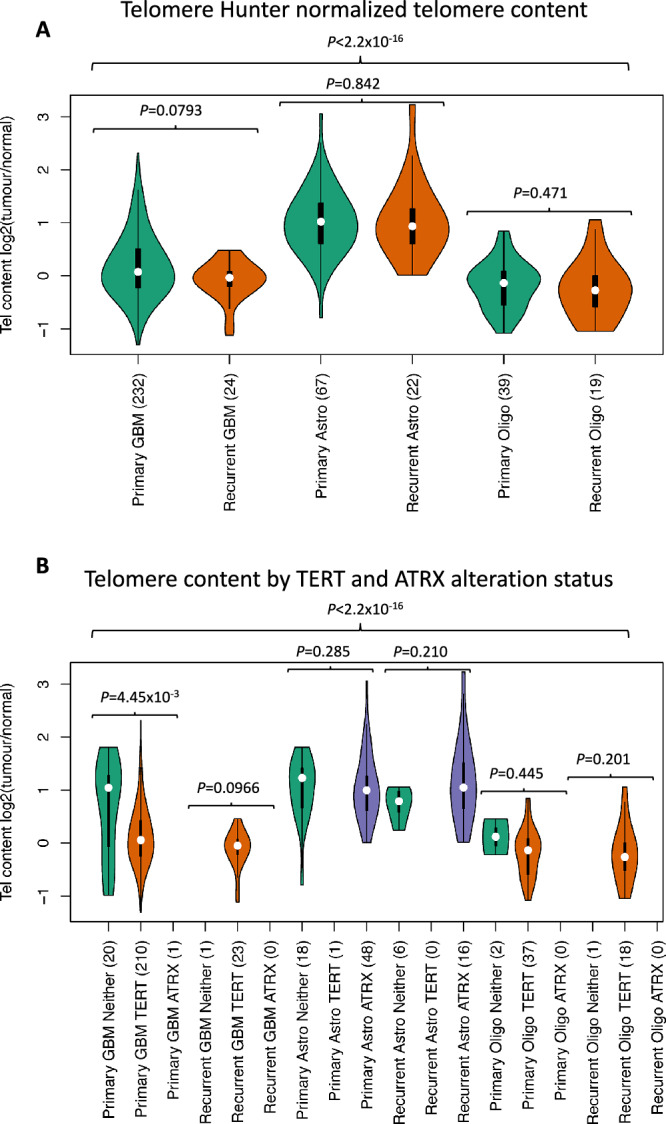
Diffuse gliomas are the commonest malignant primary brain tumour in adults. Herein, we present analysis of the genomic landscape of adult glioma, by whole genome sequencing of 403 tumours (256 glioblastoma, 89 astrocytoma, 58 oligodendroglioma; 338 primary, 65 recurrence). We identify an extended catalogue of recurrent coding and non-coding genetic mutations that represents a source for future studies and provides a high-resolution map of structural variants, copy number changes and global genome features including telomere length, mutational signatures and extrachromosomal DNA. Finally, we relate these to clinical outcome. As well as identifying drug targets for treatment of glioma our findings offer the prospect of improving treatment allocation with established targeted therapies.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures








References
-
- Crocetti, E. et al. Epidemiology of glial and non-glial brain tumours in Europe. Eur. J. Cancer48, 1532–1542 (2012). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
