

Cardiac and liver impairment on multiorgan MRI and risk of major adverse cardiovascular and liver events
- PMID: 40335668
- PMCID: PMC12283365
- DOI: 10.1038/s41591-025-03654-2
Cardiac and liver impairment on multiorgan MRI and risk of major adverse cardiovascular and liver events
Abstract
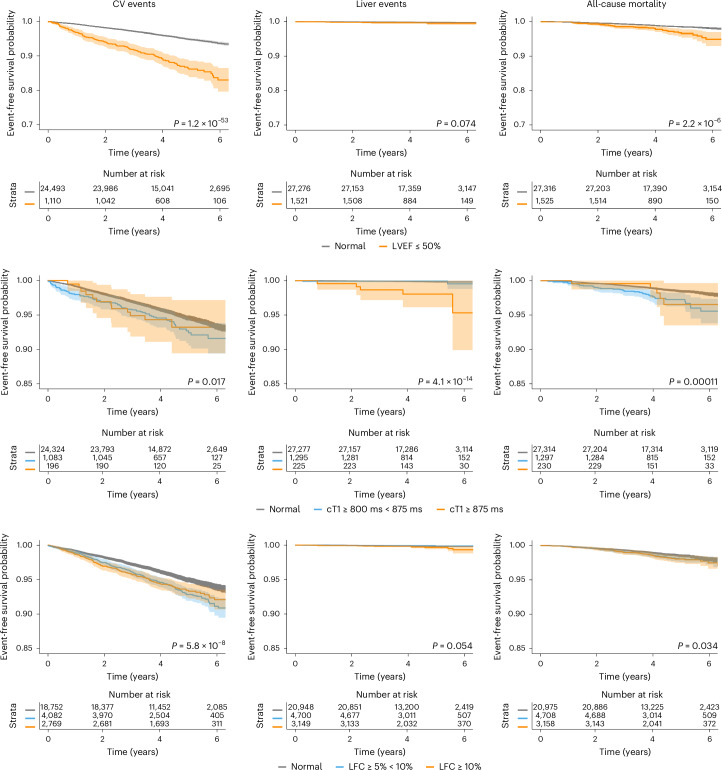
Cardiovascular disease and metabolic dysfunction-associated steatotic liver disease are common conditions associated with high mortality and morbidity, yet opportunities for integrated prevention are underinvestigated. We explored the association between impairment in the liver (defined by increased iron-corrected T1 (cT1) time) and/or heart (reduced left ventricular ejection fraction ≤ 50) and risk of experiencing cardiovascular- or liver-related events or all-cause mortality among 28,841 UK Biobank participants who underwent magnetic resonance imaging. Using Cox proportional hazard models, adjusted for age, sex, body mass index, type 2 diabetes and dyslipidaemia, we observed that cardiac impairment was associated with increased incidence of cardiovascular events (hazard ratio (HR) 2.3 (1.9-2.7)) and hospitalization (HR 2.1 (1.8-2.4)). Liver impairment was associated with incident cardiovascular hospitalization (cT1 ≥ 800 ms, HR 1.3 (1.1-1.5)), liver events (cT1 ≥ 875 ms, HR 9.2 (3.2-26) and hospitalization (cT1 ≥ 875 ms, HR 5.5 (3.2-9.3). Associations between cT1 and liver events were maintained in participants with metabolic dysfunction-associated steatotic liver disease (N = 6,223). Reduced left ventricular ejection fraction (≤50) combined with elevated cT1 (≥800 ms) were associated with earlier cardiovascular events (time to event 0.8 versus 2.4 years; P < 0.05). Cardiac and liver impairment are independently, or in combination, associated with cardiovascular or liver events, suggesting a dual role for magnetic resonance imaging in integrated prevention pathways.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: E.J., A.D. and R.B. are employees of and have shares in Perspectum Ltd. R.B. is the founder and CEO of Perspectum Ltd. The other authors declare no competing interests.
Figures


References
-
- Harrison, S. A. et al. Prospective evaluation of the prevalence of non-alcoholic fatty liver disease and steatohepatitis in a large middle-aged US cohort. J. Hepatol.75, 284–291 (2021). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
