

In Silico, Patient-Specific Assessment of Local Hemodynamic Predictors and Neointimal Hyperplasia Localisation in an Arteriovenous Graft
- PMID: 40335792
- PMCID: PMC12185642
- DOI: 10.1007/s10439-025-03737-8
In Silico, Patient-Specific Assessment of Local Hemodynamic Predictors and Neointimal Hyperplasia Localisation in an Arteriovenous Graft
Abstract
Purpose: Most computational fluid dynamics (CFD) studies on arteriovenous grafts (AVGs) adopt idealised geometries and simplified boundary conditions (BCs), potentially resulting in misleading conclusions when attempting to predict neointimal hyperplasia (NIH) development. Moreover, they often analyse a limited range of hemodynamic indices, lack verification, and fail to link the graft-altered hemodynamics with follow-up data. This study develops a novel patient-specific CFD workflow for AVGs using pathophysiological BCs. It verifies the CFD results with patient medical data and assesses the co-localisation between CFD results and NIH regions at follow-up.
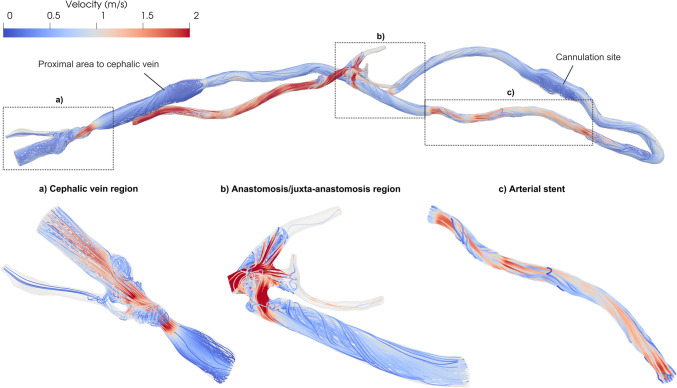
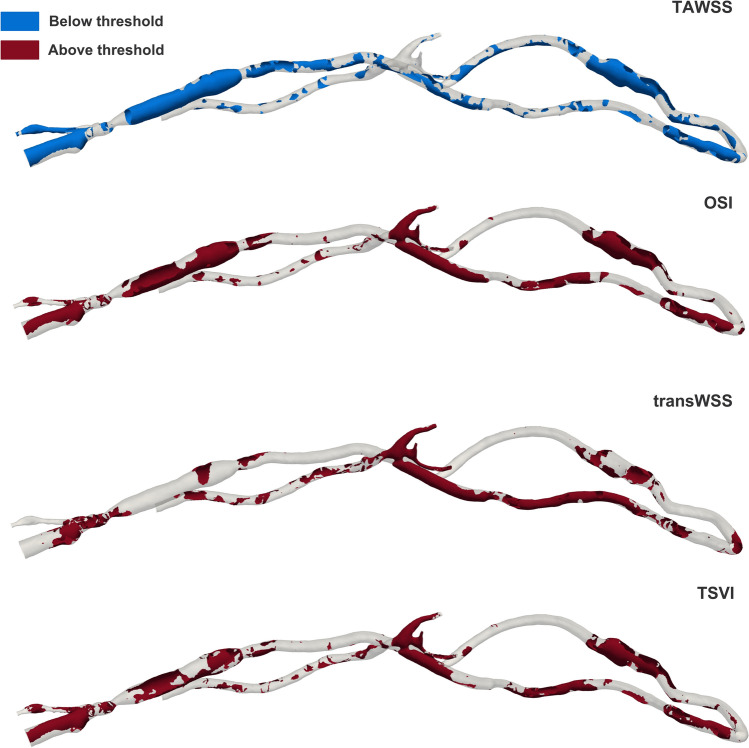
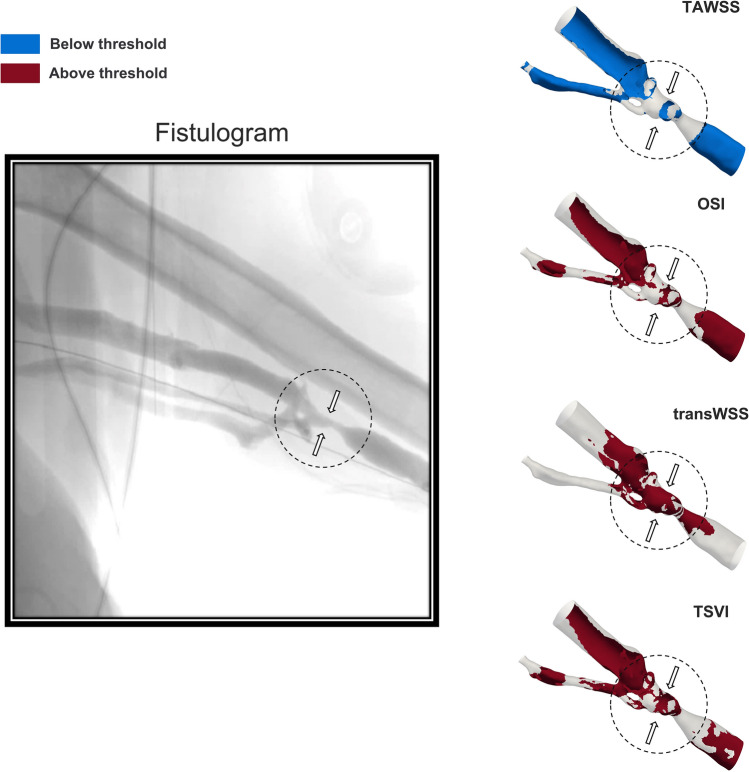
Methods: Contrast-enhanced computed tomography angiography images were used to segment the patient's AVG geometry. A uniform Doppler ultrasound (DUS)-derived velocity profile was imposed at the inlet, and three-element Windkessel models were applied at the arterial outlets of the domain. Transient, rigid-wall simulations were performed using the k-ω SST turbulence model. The CFD-derived flow waveform was compared with the patient's DUS image to ensure verification. Turbulent kinetic energy (TKE), helicity and near-wall hemodynamic descriptors were calculated and linked with regions presenting NIH from a 4-month follow-up fistulogram.
Results: In the analysed patient, areas presenting high TKE and balanced helical flow structures at baseline exhibit NIH growth at follow-up. Transverse wall shear stress index is a stronger predictor of NIH than other commonly analysed near-wall hemodynamic indices, since luminal areas subjected to high values greatly co-localise with observed areas of remodelling.
Conclusion: This patient-specific computational workflow for AVGs could be applied to a larger cohort to unravel the link between altered hemodynamics and NIH progression in vascular access.
Keywords: Arteriovenous graft; Computational fluid dynamics; Hemodynamics; Neointimal hyperplasia; Vascular access.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: The authors declare that they have no competing interests.
Figures





References
-
- Goel, N., C. Kwon, T. P. Zachariah, M. Broker, V. W. Folkert, C. Bauer, and M. L. Melamed. Vascular access placement in patients with chronic kidney disease Stages 4 and 5 attending an inner city nephrology clinic: a cohort study and survey of providers. BMC Nephrol. 2017. 10.1186/s12882-016-0431-3. - PMC - PubMed
-
- Ene-Iordache, B., and A. Remuzzi. Blood flow in idealized vascular access for hemodialysis: a review of computational studies. Cardiovasc Eng Technol. 2017. 10.1007/s13239-017-0318-x. - PubMed
-
- Konner, K. The initial creation of native arteriovenous fistulas: surgical aspects and their impact on the practice of nephrology. Semin Dial. 2003. 10.1046/j.1525-139X.2003.16064.x. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
