

From post-war reconstruction to the twenty-first century - ophthalmic pathology in Freiburg 1945-2015: review of 39,256 surgical specimens from various topographical regions collected over 71 years at a large German tertiary eye care centre
- PMID: 40335960
- PMCID: PMC12057178
- DOI: 10.1186/s12886-025-04056-1
From post-war reconstruction to the twenty-first century - ophthalmic pathology in Freiburg 1945-2015: review of 39,256 surgical specimens from various topographical regions collected over 71 years at a large German tertiary eye care centre
Abstract
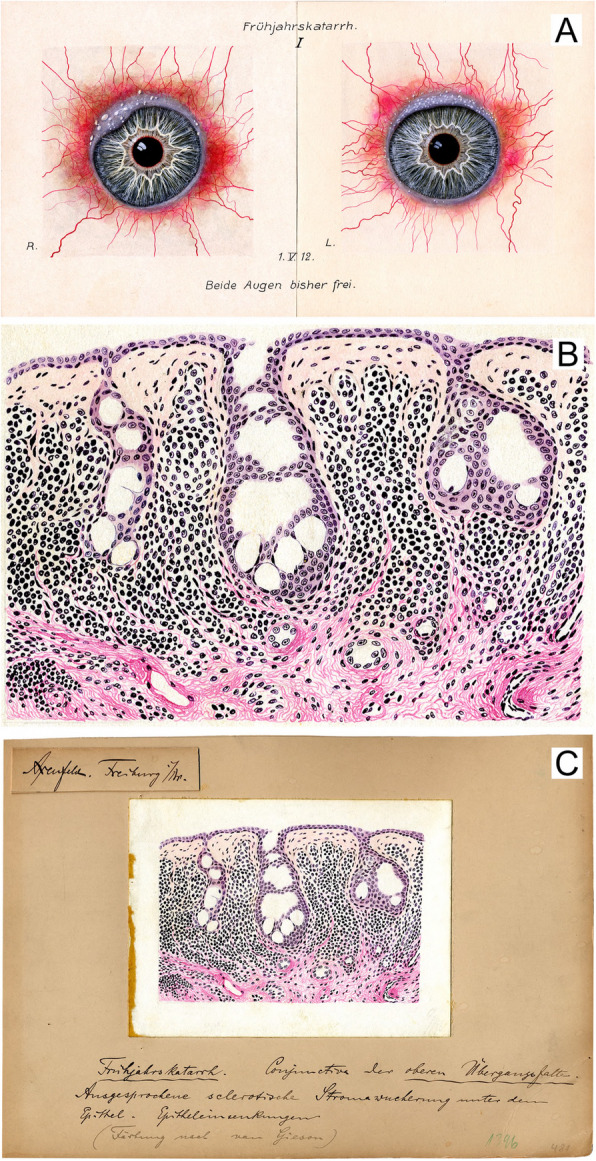
Background: Ophthalmic pathology at the Eye Center at Medical Center, University of Freiburg, Germany, looks back on a tradition of more than 150 years. Surgical specimens and associated histological diagnoses have been archived since 1945. This study is the first of its size to include 39,256 specimens examined in a single ophthalmic pathology laboratory over 71 years.
Methods: We retrospectively studied ophthalmic pathology reports and clinical records of histological specimens archived between 1945 and 2015 and compared our results with 22 studies from the literature. Samples were grouped by localisation and histopathological diagnoses assigned to various categories. Both were coded and entered into a database together with the year of surgery, patient sex and age at excision.
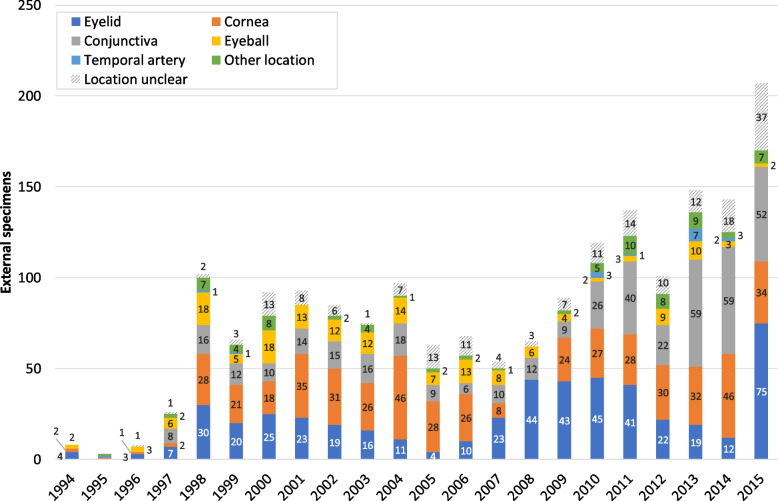
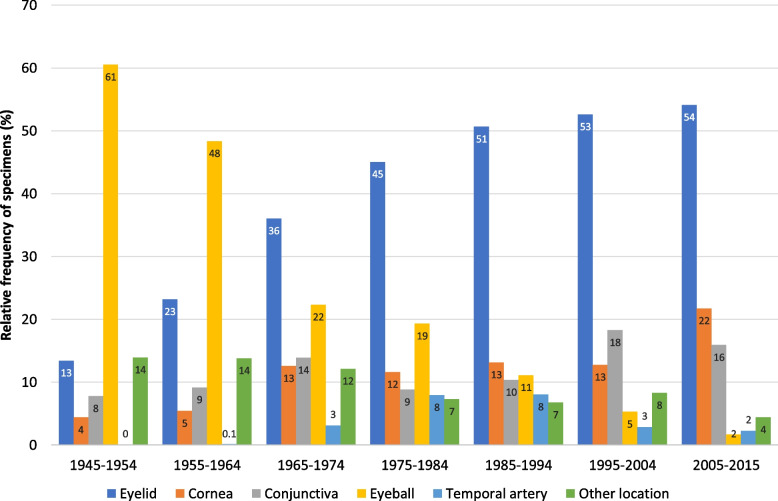
Results: The patients' age at surgery was documented in 38,845 cases (99%), of which 19,601 were female (50.5%) and 19,244 were male patients (49.5%). The bimodal frequency distribution of specimens by patient age has a similar shape to that recorded 1941-1995 for Atlanta, USA and 1959-2021 for the Swedish population. Most specimens originated from the eyelid (50%), followed by cornea (16%), conjunctiva (14%), eyeball (9.1%), temporal artery (3.9%) and other locations (6.7%) comprising 16 less frequent topographies. The proportion of eyelid (corneal, conjunctival) lesions significantly increased fourfold (fivefold, twofold) during our study period (each p < .001); that of enucleations and temporal artery biopsies decreased significantly 38- and 3.6-fold (each p < .001). Concurrently, the numbers of eyelid, corneal, conjunctival and temporal artery specimens have significantly grown (each p < .001). Annual sample numbers increased significantly across the various medical directors' tenures (1945-1967: median = 78; 1968-1987: median = 454; 1988-2002: median = 670; 2003-2015: median = 1,445) (p < .001).
Conclusions: Historical events, general population developments and new surgical techniques and treatment options caused changes in the occurrence of various ocular and periocular specimens. Our study data contribute to providing an overall picture of the nature and relative frequency of ocular conditions leading to surgical excision of specimens with subsequent histopathological examination. A continuous sharp increase in case numbers since 1987 clearly exceeds the demographic trend emphasising the ever-growing importance of the sub-speciality of ophthalmic pathology. Ideally, histopathological assessments should be conducted by experienced ophthalmologists with surgical and pathology expertise, or by experienced pathologists with ophthalmology expertise, to ensure optimal patient care.
Keywords: Conjunctiva; Cornea; Eyeball; Eyelid; Ophthalmic pathology; Temporal artery; Time trends.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: No names, personal identification numbers, home addresses, contact information, photographs, or any other data that could be traced back to individual patients were collected. This study was approved by the Ethics Committee at the University of Freiburg Medical Center on 30 July 2019 (reference number: 212/19), waiving documentation of informed consent due to the retrospective nature of the study using no sensitive patient information but anonymous clinical data only. The study was conducted in accordance with the principles of Article 35 of the Helsinki Declaration. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures






References
-
- Rohrbach JM, Auw-Hädrich C, Messmer EM, et al. Zur Situation der Ophthalmopathologie in Deutschland: eine aktuelle Bestandsaufnahme. Klin Monatsbl Augenheilkd. 2009;226:740–6. - PubMed
-
- Rohrbach JM. Albrecht von Graefe (1828–1870) und die Ophthalmopathologie. Klin Monatsbl Augenheilkd. 2015;232:1101–4. - PubMed
-
- Herwig-Carl MC, Löffler KU. Goldstandard Ophthalmopathologie – noch zeitgemäß? [Ophthalmic Pathology - Still the Gold Standard?]. Klin Monbl Augenheilkd. 2020;237(7):867–78. - PubMed
-
- Lang GK, Deutsche Ophthalmopathologen (DOP). Der Ophthalmopathologe im klinischen Einsatz [The Ocularpathologist in Everday Clinical Routine]. Klin Monbl Augenheilkd. 2015;232(12):1361–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
