

Optimal timing for cholecystectomy: unveiling insights from a decade-long study on acute cholecystitis and symptomatic cholecystolithiasis
- PMID: 40336005
- PMCID: PMC12060486
- DOI: 10.1186/s12893-025-02851-7
Optimal timing for cholecystectomy: unveiling insights from a decade-long study on acute cholecystitis and symptomatic cholecystolithiasis
Abstract
Background: Acute calculus cholecystitis affects 10 to 20% of untreated individuals. Thus, the surgical community has argued for decades over whether an earlier or later cholecystectomy is better for this condition.
Objectives: To compare surgical results, morbidity, and mortality and determine the best timing for surgical intervention among patients with gallstones.
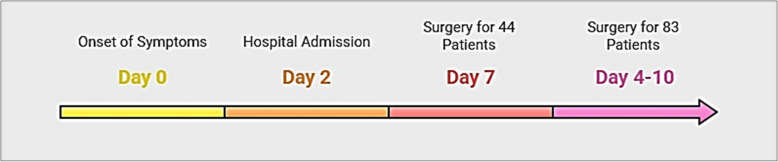
Patients and methods: This prospective cohort study was conducted in Erbil Teaching Hospital, Erbil, Iraq, from January 2013 to December 2023 on 767 patients with acute cholecystitis or symptomatic cholecystolithiasis. Patients underwent various types of cholecystectomy (early, intermediate, late, and elective) based on when surgery was conducted after the onset of symptoms. Then, medical treatments were advised, and they were followed up for six weeks. Finally, patients' physical health, postoperative infection severity and complications were assessed, despite reporting patients' age, gender, operation type, chances of conversions, durations of procedure, and hospital stay.
Results: Most patients were females (72.1%), experienced laparoscopic technique (98.44%), and had ASA II (n = 548, 71.44%). The mean age of patients was 48.40 ± 67.14 years, the mean operation time was 50 ± 30.89 min, and the mean hospitalization time before and after operation was 1.0 ± 0.47 and 2.75 ± 1.63 days, respectively. Most patients from the intermediate group (n = 83) opted for a postponed strategy. Chronic inflammation (grade 0 infection severity) was highest in most patients of the delayed (67.2%) and intermediate groups (53.01%). Most patients had no complications (score 0), and the least had severe complications.
Conclusion: Delayed surgical intervention was harmless and may even be superior to immediate treatment for acute cholecystitis. The morbidity and mortality hazard remains high even in the most severe cases, especially for individuals who received early and intermediate therapy.
Keywords: Acute cholecystitis; Cholecystolithiasis; Gallstones; Laparoscopic cholecystectomy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All procedures, including patient selection and data collection, were approved by the Ethical Committee of the College of Medicine, Hawler Medical University, Erbil, Iraq. Before any of it occurred, written informed consent was obtained from the patients for the surgery, research participation, and publication of results. The Helsinki Declaration of 1964 and its later revisions were followed throughout all study phases to ensure the highest level of ethical conduct. The hospital admission consent already included provisions for protecting patient data and authorization for the data review process. Consent for publication: Not applicable, no personal information or images of any kind are included in the research. Requested access to the raw data used in this study will not reveal any personally identifiable information about any participant. Competing interests: The authors declare no competing interests.
Figures

References
-
- Rajah KH. Acute Cholecystitis: An Update. 2024:127–137.
MeSH terms
LinkOut - more resources
Full Text Sources
