

Does the surgeon's learning curve impact pentafecta outcomes in radical prostatectomy? a systematic review and meta-analysis
- PMID: 40336044
- PMCID: PMC12060569
- DOI: 10.1186/s12894-025-01810-x
Does the surgeon's learning curve impact pentafecta outcomes in radical prostatectomy? a systematic review and meta-analysis
Abstract
Introduction: Radical prostatectomy is a key treatment for prostate cancer. However, the impact of the learning curve of the surgeon has on the pentafecta is unclear. This meta-analysis aims to determine the impact of a procedure being performed in the initial learning curve has on the surgical results.
Materials and methods: A systematic review of MEDLINE, Embase, Scopus, Web of Science, and Google Scholar was conducted up to March 2024, focusing on learning curves in prostatectomy. Primary outcome was biochemical recurrence rate (BCR); secondary outcomes included positive surgical margin (PSM) rate, continence, potency, operative time, blood loss, and complications (Clavien-Dindo classification). Bias was assessed using the ROBINS-I tool, and statistical analysis was done via Review Manager 5.4.
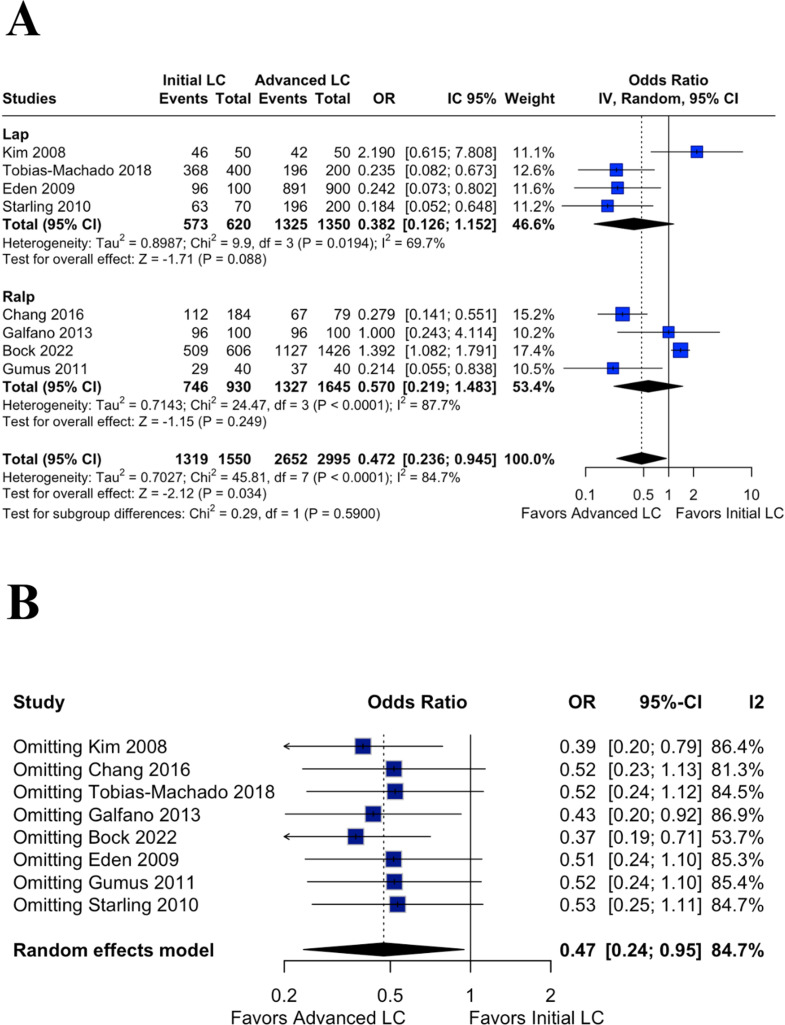
Results: Sixteen studies with 21,851 patients were included. No significant difference in BCR rates was found between initial and advanced learning curves (OR1.44;95%CI0.97,2.13;p = 0.07;I²=74%). No significant difference in continence rates was also observed. (RD-0.05;95CI-0.10,0.01;p = 0.08;I²=86%). However, advanced learning curves showed lower PSM rates (OR1.61;95%CI1.19,2.17;p = 0.002;I²=88%), higher potency, less blood loss, shorter operative time, and fewer complications. Although randomized trials are unlikely in this context, further high-quality prospective studies are needed to validate these findings.
Conclusion: This meta-analysis highlights that achieving favorable outcomes in key pentafecta parameters-particularly potency, continence, and complication rates-increases with surgical experience. These findings emphasize the value of structured mentorship and establishing surgical volume benchmarks in training programs. Our analysis suggests that reaching a threshold of 100 cases may be necessary to consistently attain optimal functional and perioperative results.
Keywords: Learning curve; Meta-analysis; Prostatectomy; Robotic surgical procedures; laparoscopy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Human ethics and consent to participate declarations: Not applicable. Competing interests: The authors declare no competing interests.
Figures









References
-
- Artibani W, Fracalanza S, Cavalleri S, et al. Learning curve and preliminary experience with Da Vinci-assisted laparoscopic radical prostatectomy. Urol Int. 2008;80:237–44. - PubMed
-
- Vickers AJ, Bianco FJ, Serio AM, et al. The surgical learning curve for prostate cancer control after radical prostatectomy. J Natl Cancer Inst. 2007;99:1171–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
