

The effects of prolonged prone positioning on response and prognosis in patients with acute respiratory distress syndrome: a retrospective cohort study
- PMID: 40336057
- PMCID: PMC12057286
- DOI: 10.1186/s40560-025-00795-x
The effects of prolonged prone positioning on response and prognosis in patients with acute respiratory distress syndrome: a retrospective cohort study
Abstract
Background: Prone positioning improves outcomes in patients with acute respiratory distress syndrome (ARDS), but the optimal duration in critical care settings remains uncertain. This study aims to evaluate the investigates the impact of prone ventilation duration on clinical outcomes.
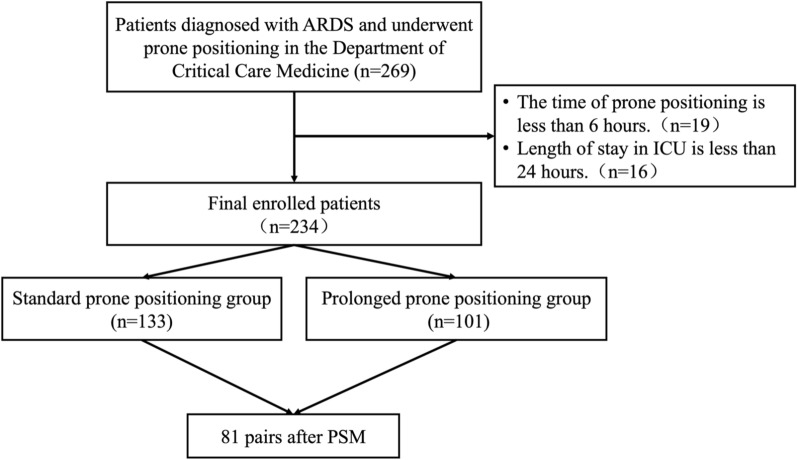
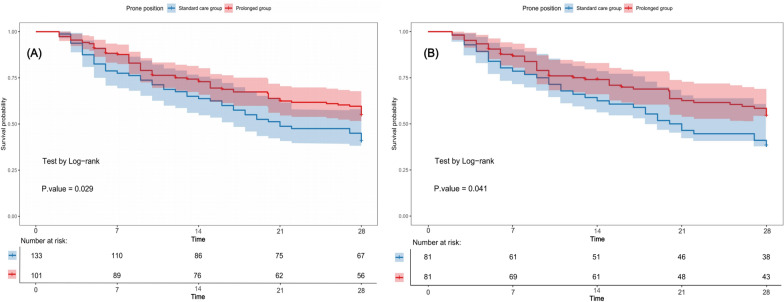
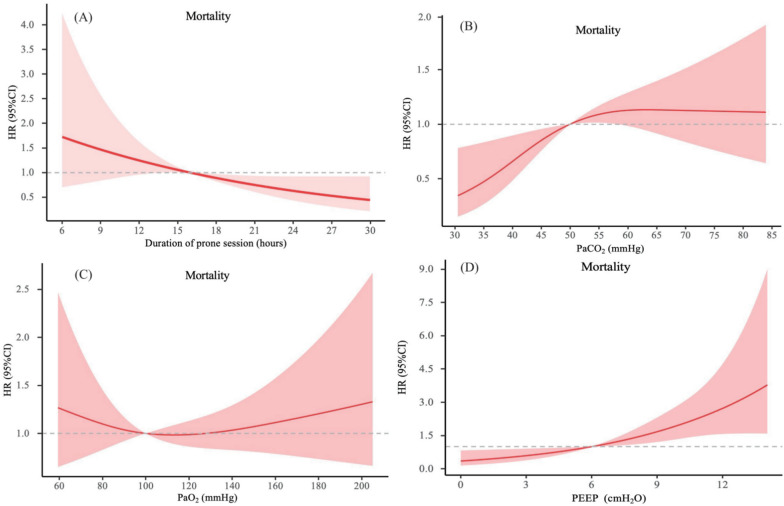
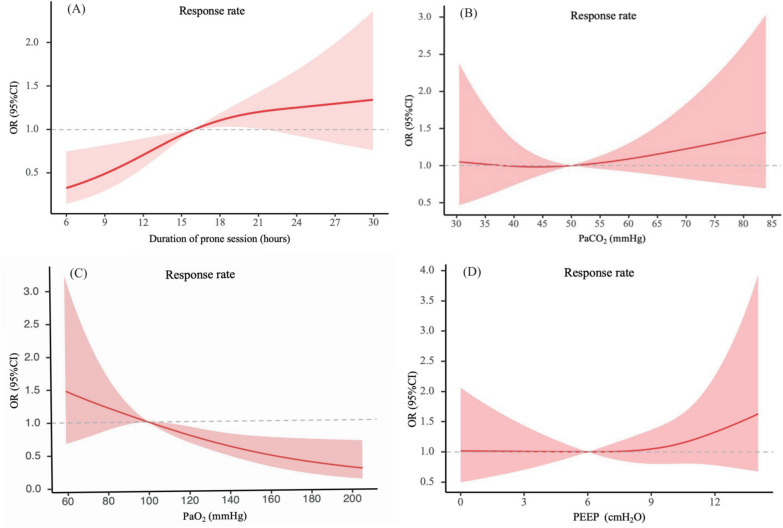
Methods: This retrospective study was conducted on ARDS patients admitted to the intensive care unit (ICU), Nanfang hospital of Southern Medical University, who received prone positioning. Patients were categorized into two groups: the prolonged prone positioning (PPP) (≥ 16 h) group and the standard prone positioning (SPP) (< 16 h) group. Propensity score matching (PSM) was employed to balance baseline characteristics. Cox proportional hazards, regression models were utilized to evaluate the association between the prone duration and clinical outcomes. Kaplan-Meier survival curves were generated to compare 28-day mortality, with log-rank tests analyzing differences. Restricted cubic spline (RCS) were applied to investigate the time-response between prone duration, PaCO₂, PaO₂, positive end-expiratory pressure, response rate, and 28-day mortality. In addition, the incidence of prone position-related complications was assessed in both groups.
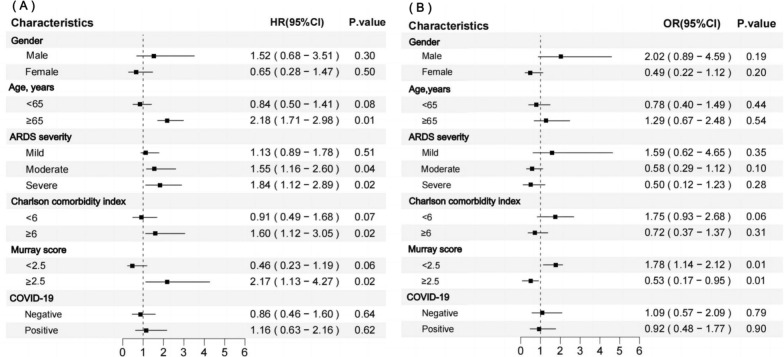
Results: A total of 234 patients with ARDS were included, with an overall 28-day mortality of 49.1% (115/234). After PSM, 81 matched pairs were compared. The PPP group had lower 28-day mortality (46.9% vs. 53.1%; hazard ratios (HR): 0.53; 95% CI 0.32-0.85; P = 0.033) and improved prone positioning response rate [70.5% vs. 60.5%; odds ratio (OR): 1.46; 95% CI 1.23-1.89; P = 0.025]. RCS analysis suggested a reduction in mortality with prone durations ≥ 16 h, and longer durations correlated with better prone response. However, no significant association was found between PPP and reduced ICU or hospital length of stay. RCS analysis indicated a gradual decrease in 28-day mortality with increasing duration of prone positioning, and longer duration were associated with a higher likelihood of a prone response. There were no significant differences in prone ventilation-related complications between the two groups.
Conclusions: PPP (≥ 16 h) is associated with reduced 28-day mortality and improved response rates in ICU patients with ARDS, without increasing complication risks. Prospective studies are needed to further validate these results.
Keywords: Acute respiratory distress syndrome; Intensive care unit; Prognosis; Prolonged prone position; Response rates.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Ethics Commission of Nanfang Hospital (NFEC-202312-K61). The Ethics Commission of Nanfang Hospital waived the requirement for obtaining informed consent. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–33. - PubMed
Grants and funding
- 82302411/National Natural Science Foundation of China
- 2021A1515220003/Basic and Applied Basic Research Foundation of Guangdong Province
- 2021A1515111028/Basic and Applied Basic Research Foundation of Guangdong Province
- 2025A04J4187/Science and Technology Program of Guangzhou
- 2023CR018/Initiative Project of Clinical Research of Southern Medical University
LinkOut - more resources
Full Text Sources
Miscellaneous
