

A comparison between the self-report of chronic cardiovascular diseases with health insurance data: insights from the population-based LIFE-Adult study
- PMID: 40336119
- PMCID: PMC12057059
- DOI: 10.1186/s13690-025-01606-3
A comparison between the self-report of chronic cardiovascular diseases with health insurance data: insights from the population-based LIFE-Adult study
Abstract
Background: Self-reporting is a common approach in observational epidemiological studies. However, information can be biased by several causes and can, therefore, affect the outcomes of the investigations. This analysis aimed to evaluate the agreement between self-reported data from a population-based cohort study with data from two large German health insurance companies.
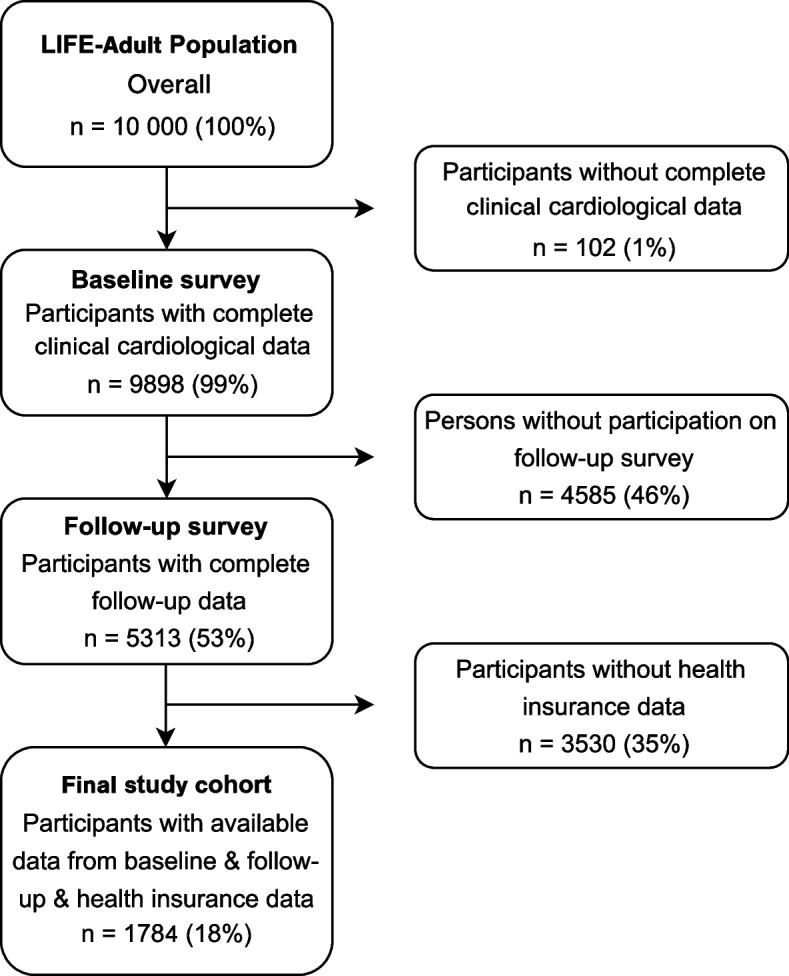
Methods: Participants with available self-reported diagnoses of a history of stroke, atrial fibrillation (AF), heart failure (HF), and myocardial infarction (MI) from the baseline and the follow-up (after six years) surveys of the prospective population-based LIFE-Adult study were included in this study. Two health insurance companies provided ICD-10-GM codes. The agreement between the self-reports and health insurance data (HID) was examined by calculating sensitivity, specificity, Cohen`s Kappa, positive and negative predictive values. We used multivariable logistic regression models to examine whether odds ratios (OR) for the association between risk factors and the certain disease changed, depending on whether self-reports or HID was used as the dependent variable.
Results: One thousand seven hundred eighty four individuals with complete data were included in this interim analysis. Mean age was 58 (SD±12) years and 984 (55%) were female. 52 (2.9%) subjects reported a history of stroke, 99 (5.6%) AF, 63 (3.5%) HF, and 46 (2.6%) MI. Compared with the HID, a high specificity was found for all four diagnoses (stroke: 99% [95% CI 99.3-99.9]; AF: 99% [95% CI 98.1-99.2], HF: 98% [95% CI 97.6-98.9], and MI: 99% [95% CI 98.9-99.7]). Sensitivity ranged from 58% (95% CI 47.4-69.5) for stroke over 61% (95% CI 48.8-74.0) for MI, to 65% (95% CI 56.6-73.9) for AF. Sensitivity in HF was the lowest (20% [95% CI 14.4-26.5]).
Conclusion: The use of German health insurance data is a feasible method for verifying population-based self-reported diagnoses. The sensitivity varied among the self-reported diseases compared with the health insurance data, whereas the specificity was continuously high. The verification of self-reported diagnoses using health insurance data as an additional data source may be considered in future population-based assessments to reduce misclassification error of self-reported data.
Keywords: Agreement; Atrial fibrillation; Health insurance; Heart failure; Myocardial infarction; Population-based; Self-report; Stroke; Validation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All participants provided written and signed consent forms prior to the baseline investigations. The study was approved by the local Ethics Committee on the Medical Faculty at Leipzig University and is in accordance with the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Nationwide Analysis (2016-2020) of the Burden of Thrombocytopenia on Patients Admitted Due to Myocardial Infarction, Heart Failure or Atrial Fibrillation.Cureus. 2025 Feb 3;17(2):e78452. doi: 10.7759/cureus.78452. eCollection 2025 Feb. Cureus. 2025. PMID: 40051938 Free PMC article.
-
The predictive value of estimated glucose disposal rate and its association with myocardial infarction, heart failure, atrial fibrillation and ischemic stroke.Diabetes Obes Metab. 2025 Mar;27(3):1359-1368. doi: 10.1111/dom.16132. Epub 2025 Jan 2. Diabetes Obes Metab. 2025. PMID: 39743837
-
Risk of early mortality and cardiovascular disease in type 1 diabetes: a comparison with type 2 diabetes, a nationwide study.Cardiovasc Diabetol. 2019 Nov 16;18(1):157. doi: 10.1186/s12933-019-0953-7. Cardiovasc Diabetol. 2019. PMID: 31733656 Free PMC article.
-
Cardiovascular outcomes in breast cancer survivors: a systematic review and meta-analysis.Eur J Prev Cardiol. 2023 Dec 21;30(18):2018-2031. doi: 10.1093/eurjpc/zwad243. Eur J Prev Cardiol. 2023. PMID: 37499186
-
Cardiovascular outcomes associated with SGLT-2 inhibitors versus other glucose-lowering drugs in patients with type 2 diabetes: A real-world systematic review and meta-analysis.PLoS One. 2021 Feb 19;16(2):e0244689. doi: 10.1371/journal.pone.0244689. eCollection 2021. PLoS One. 2021. PMID: 33606705 Free PMC article.
References
-
- Vaduganathan M, Mensah GA, Turco JV, Fuster V, Roth GA. The Global Burden of Cardiovascular Diseases and Risk: A Compass for Future Health. J Am Coll Cardiol. 2022;80:2361–71. - PubMed
-
- Okura Y, Urban LH, Mahoney DW, Jacobsen SJ, Rodeheffer RJ. Agreement between self-report questionnaires and medical record data was substantial for diabetes, hypertension, myocardial infarction and stroke but not for heart failure. J Clin Epidemiol. 2004;57:1096–103. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
