

Clinical risk factors for postoperative infection in adult cardiac surgery with cardiopulmonary bypass: a retrospective study
- PMID: 40336598
- PMCID: PMC12056962
- DOI: 10.1016/j.infpip.2025.100458
Clinical risk factors for postoperative infection in adult cardiac surgery with cardiopulmonary bypass: a retrospective study
Abstract
Background: Postoperative infection remains a serious problem for patients undergoing open-heart surgery and is associated with poor prognosis and mortality.
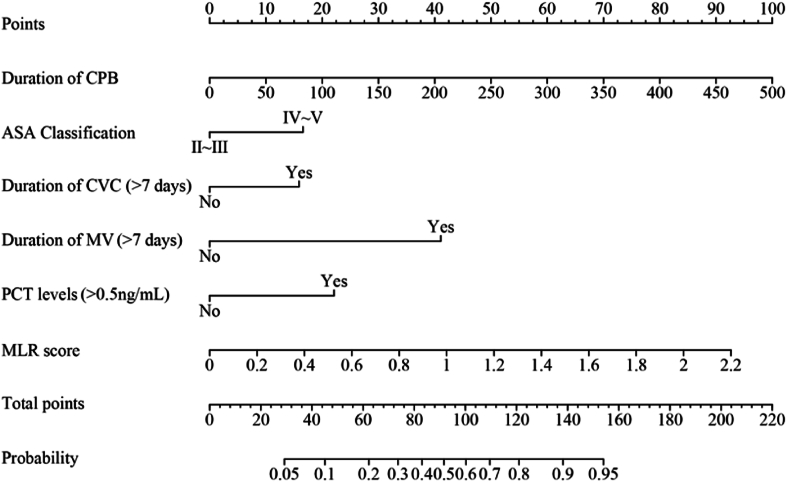
Aim: To determine the incidence, characteristics and associated risk factors for nosocomial infections in adult cardiac surgery patients and to develop a nomogram prediction model.
Methods: Data were retrospectively collected from patients who underwent cardiac surgery with cardiopulmonary bypass (CPB) at a tertiary hospital in 2023. Patients were divided into an infected group (N = 130) and a non-infected group (N = 192). Multivariate logistic regression analysis was used to analyse the independent risk factors for healthcare-associated infections after cardiac surgery under CPB.
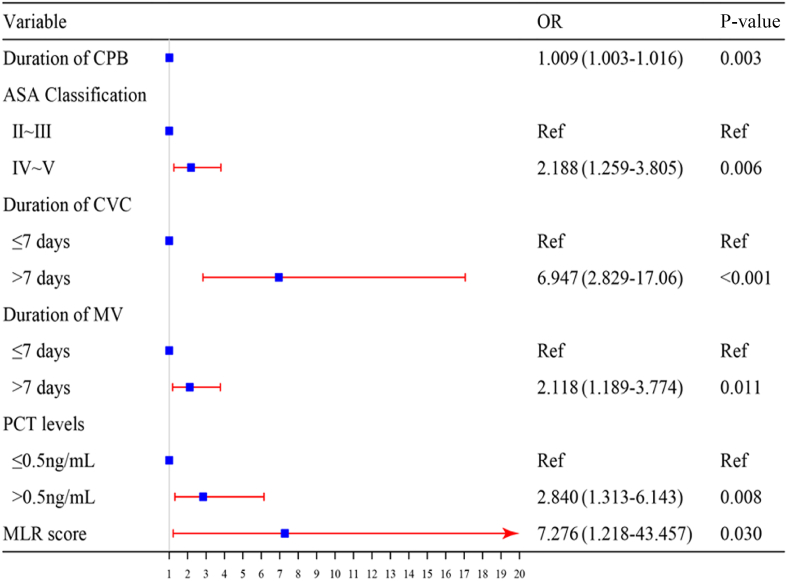
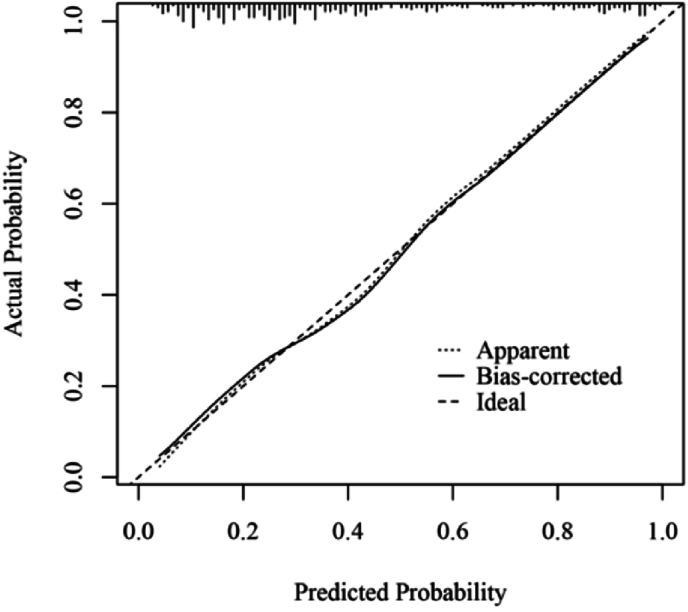
Results: Of the 1584 patients, 130 (8.21%) developed postoperative infections (infection group). Lower respiratory tract was the most common site of infection (N = 74, 56.9%), while Gram-negative bacteria were the predominant isolates overall (N = 81, 62.3%). Among the Gram-negative bacteria, Acinetobacter baumannii was the most frequently identified, whereas Staphylococcus aureus was the leading strain among Gram-positive bacteria. Multivariate logistic regression analysis of the 322 patients included in the study revealed that CPB duration, American Society of Anaesthesiologists score, procalcitonin concentration on the first postoperative day, monocyte:lymphocyte ratio, preinfection mechanical ventilation duration, and preinfection central venous catheterization duration were the six independent predictors of postoperative infection. The area under the receiver operating characteristic curve was 0.824 (0.778-0.870), and the model showed good predictive performance.
Conclusion: A nomogram has been developed to predict postoperative infection via commonly available data. This tool could assist clinicians in optimising the perioperative care of patients undergoing cardiac surgery with CPB, but further external validation is needed.
Keywords: Cardiac surgery; Cardiopulmonary bypass; Nomogram; Postoperative infection; Risk factors.
© 2025 The Authors.
Conflict of interest statement
None declared.
Figures



Similar articles
-
[High preoperative pulmonary artery systolic pressure is associated with acute kidney injury and prognosis in patients underwent cardiopulmonary bypass surgery].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Mar;32(3):319-323. doi: 10.3760/cma.j.cn121430-20200224-00073. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32385996 Chinese.
-
The Characterization of Postoperative Mechanical Respiratory Requirement in Neonates and Infants Undergoing Cardiac Surgery on Cardiopulmonary Bypass in a Single Tertiary Institution.J Cardiothorac Vasc Anesth. 2022 Jan;36(1):215-221. doi: 10.1053/j.jvca.2021.04.023. Epub 2021 Apr 25. J Cardiothorac Vasc Anesth. 2022. PMID: 34023203
-
Nomogram for intraoperatively acquired pressure injuries in children undergoing cardiac surgery with cardiopulmonary bypass: a retrospective study.BMC Pediatr. 2024 Aug 8;24(1):510. doi: 10.1186/s12887-024-04989-4. BMC Pediatr. 2024. PMID: 39118018 Free PMC article.
-
Development and validation of a prediction model for acute kidney injury following cardiac valve surgery.Front Med (Lausanne). 2025 Jan 31;12:1528147. doi: 10.3389/fmed.2025.1528147. eCollection 2025. Front Med (Lausanne). 2025. PMID: 39958823 Free PMC article.
-
Risk factors for venoarterial-extracorporeal membrane oxygenation related nosocomial infection in children after cardiac surgery.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022 Jun 28;47(6):748-754. doi: 10.11817/j.issn.1672-7347.2022.210472. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35837774 Free PMC article. Chinese, English.
Cited by
-
Risk factor analysis and predictive model development for healthcare-associated infections post-coronary artery bypass grafting.Front Public Health. 2025 Jul 3;13:1605272. doi: 10.3389/fpubh.2025.1605272. eCollection 2025. Front Public Health. 2025. PMID: 40678649 Free PMC article.
References
-
- Baehner T., Boehm O., Probst C., Poetzsch B., Hoeft A., Baumgarten G., et al. Kardiopulmonaler bypass in der Herzchirurgie. Anaesthesist. 2012;61:846–856. - PubMed
-
- Massart N., Mansour A., Ross J.T., Piau C., Verhoye J.P., Tattevin P., et al. Mortality due to hospital-acquired infection after cardiac surgery. J Thorac Cardiovasc Surg. 2022;163:2131–2140.e3. - PubMed
-
- de la Varga-Martínez O., Gómez-Sánchez E., Muñoz M.F., Lorenzo M., Gómez-Pesquera E., Poves-Álvarez R., et al. Impact of nosocomial infections on patient mortality following cardiac surgery. J Clin Anesth. 2021;69 - PubMed
-
- Kollef M.H., Sharpless L., Vlasnik J., Pasque C., Murphy D., Fraser V.J. The impact of nosocomial infections on patient outcomes following cardiac surgery. Chest. 1997;112:666–675. - PubMed
LinkOut - more resources
Full Text Sources
