

Innovative Ultrasound-Guided Erector Spinae Plane Nerve Block Model for Training Emergency Medicine Physicians
- PMID: 40336693
- PMCID: PMC12054114
- DOI: 10.21980/J8PW7D
Innovative Ultrasound-Guided Erector Spinae Plane Nerve Block Model for Training Emergency Medicine Physicians
Abstract
Audience: This ultrasound-guided erector spinae plane (ESP) nerve block model is designed to instruct emergency medicine (EM) attending and resident physicians. However, this innovation is appropriate for all levels of learners, including medical students, advanced practice clinicians (APCs), and clinicians in other medical specialties.
Introduction: The ESP nerve block is a relatively new regional anesthesia technique that involves injection of local anesthetic along the fascial plane below the erector spinae muscles.1-3 The ESP nerve block was first described in 2016 by Forero et al. to help manage severe thoracic neuropathic pain resulting from malunion of multiple rib fractures and metastatic disease of the ribs.1 The block has since emerged as a safe, feasible and effective analgesic intervention for various pathologies, including management of pain for acute rib fractures.2,3 However, barriers to implementation into routine practice in the emergency department (ED) exist due to gaps in knowledge about the block and a lack of training.4 We created a novel, inexpensive, and portable ultrasound-guided ESP nerve block model that can be used to facilitate training for EM physicians and residents.
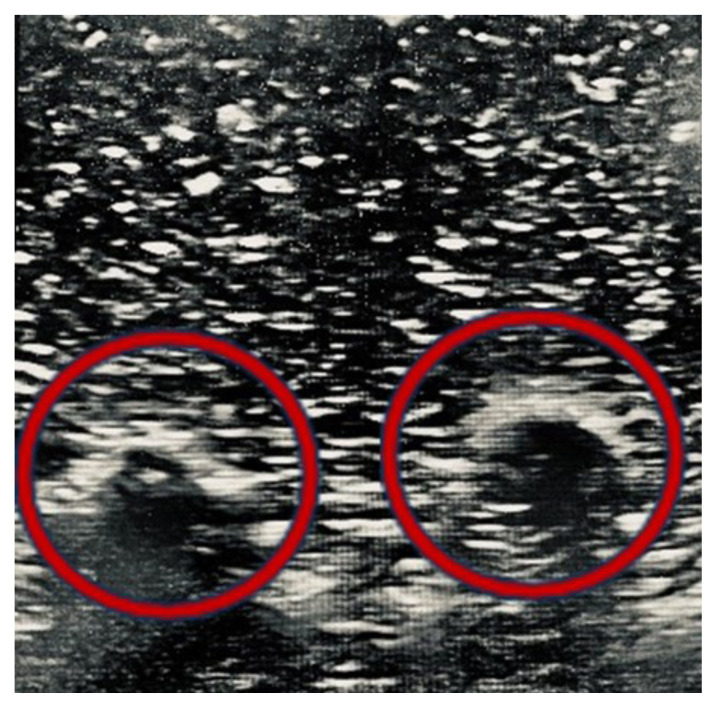
Educational objectives: This innovation model is designed to facilitate hands-on training of the ultrasound-guided ESP nerve block using a practical, realistic, and cost-effective ballistics gel model. By the end of this training session, learners should be able to: 1) identify relevant sonoanatomy on the created simulation model; 2) demonstrate proper in-plane technique; and 3) successfully replicate the procedure on a different target on the created training model.
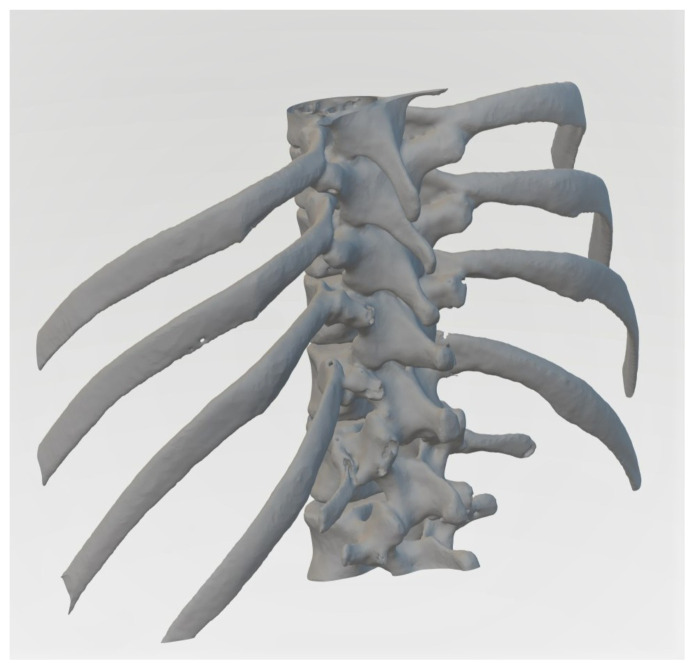
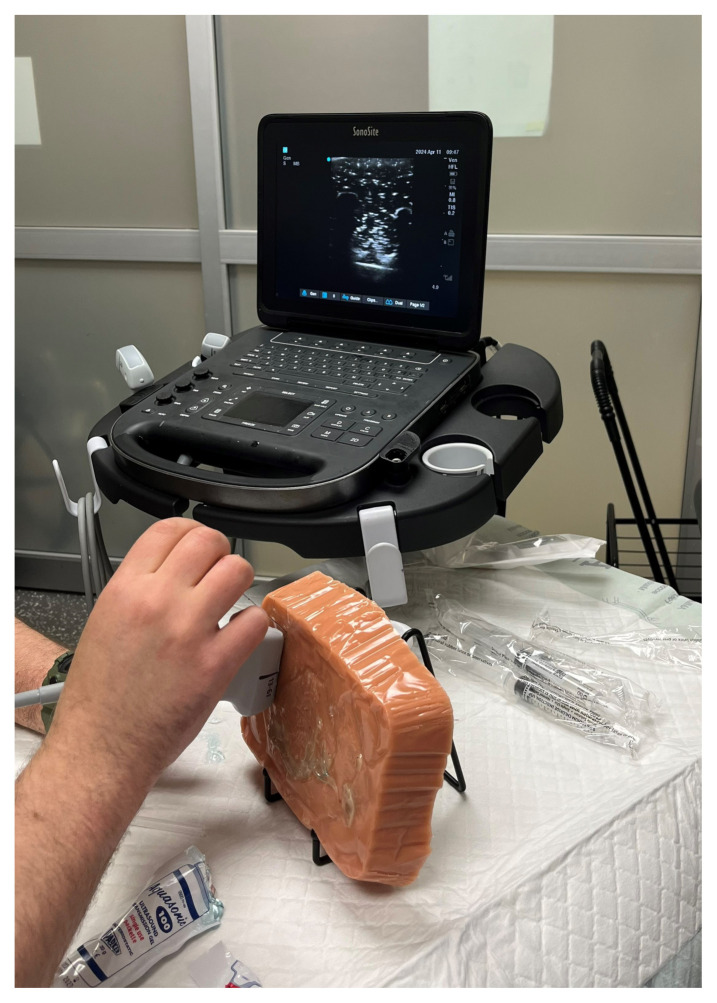
Educational methods: We created a cost-effective ESP nerve block model using a 3-D printed spine and ribcage suspended in ballistics gel that is compatible with ultrasound. The use of ballistics gelatin in the model closely simulates the viscosity and density of animal tissue, allows for ultrasound use, and is cost-efficient and more feasible than other organic models because it can be easily melted and re-used.5 At the time of this model's creation, the only previous approach to creating an ESP model was a porcine model that used meat cuts from the lower thoracic region and spine. However, the major limitation of this porcine model was its limited shelf life.6 The created ESP model was incorporated into a hands-on training module that took place one to two times per week over two months. Additional sessions were incorporated on a case-by-case basis. All participants were first given access to an educational ESP Nerve Block PowerPoint presentation to be reviewed prior to attending in-person sessions. The training sessions were promoted through weekly email reminders containing the dates and a link to an online sign-up sheet. Additionally, on training days, our project director actively sought to recruit available participants on-shift. Each training day, a one-to-two-hour window was made available for participants to attend. Each training session was conducted with a small group of four or fewer trainees beginning with a short didactic lecture presented by a lead instructor, either the Associate Research Director of Emergency Medicine or the Medical Director for Division of Pain Medicine, followed by live demonstration of the nerve block using the ESP model. Participants were then given the opportunity to practice on the ESP model. Sessions ended when all participants demonstrated proper and successful technique with the model, reported adequate confidence with the block, and all questions were addressed. Feedback on technique was provided throughout the training session by the lead instructor.
Research methods: Post-education surveys were distributed to all participants electronically to assess training impact. The survey collected data on the participants' title, prior experience performing ESP nerve blocks, competency of the teaching model, and their comfort with performing the block after the training. The Institutional Review Board (IRB) reviewed and deemed this project exempt from full board review.
Results: Thirty-four participants attended the in-person training sessions, consisting mainly of EM attending (16/34; 47%) and resident (13/34; 38%) physicians. Fourteen (14/34; 41%) participants returned completed surveys, of which 50% were residents (7/14; 50%) and 50% attending physicians (7/14; 50%). The majority (12/14; 86%) of respondents reported no prior experience in performing an ESP block with only 14% (2/14; 14%) reporting performing fewer than two ESP nerve blocks per year. All respondents (14/14; 100%) agreed or strongly agreed that the education session with the ESP model improved their confidence, knowledge, and skills to perform the block. All (14/14; 100%) agreed or strongly agreed that they felt confident in their ability to use ultrasound to identify landmarks on the model pertinent to performing the ESP block. All (14/14; 100%) reported that they felt that the material presented during these training sessions was relevant to their practice in the ED, within their scope of practice, and part of their job as an ED physician. All (14/14; 100%) reported they felt performing ESP blocks in the ED could positively impact patient outcomes and reported an increased likelihood of performing the ESP block in the ED following this training session. Lastly, respondents were asked to list any barriers that might inhibit them from performing the ESP block on shift, in addition to any strategies to facilitate ESP block use. Four participants (4/14; 29%) reported barriers to performing an ESP block including time constraints (50%) and patient mobility limitations (50%). Twelve participants (12/14; 86%) reported facilitators to performing ESP blocks, the most common of which being easier access to supplies and assistance with procedure setup (43%), followed by increased education sessions (21%).
Discussion: Our survey results indicate that our learners perceived an increase in knowledge, confidence, and skills in performing ultrasound-guided ESP blocks after using our innovative model as a hands-on teaching tool during a training session. A simple 30-minute training session with a novel ballistics gelatin ESP model can improve confidence, knowledge, and skills in performing this block in the ED, even amongst nerve block naive physicians. Additionally, by identifying barriers to the use of the ESP block in the ED, researchers can create strategies to mitigate these challenges to increase utilization of these procedures for appropriate patients in the ED. These strategies include but are not limited to addressing ways to mitigate time constraint issues, patient mobility limitations, access to supplies, assistance with procedure set up, and increasing education sessions to increase physician comfort with successful completion of the procedure.
Topics: Erector spinae plane nerve block, ultrasound, regional anesthesia, rib fractures, ballistics gel model, hands-on training.
© 2025 Correa Ibarra, et al.
Figures







References
LinkOut - more resources
Full Text Sources
Miscellaneous