

Post-exertional malaise in Long COVID: subjective reporting versus objective assessment
- PMID: 40337174
- PMCID: PMC12055772
- DOI: 10.3389/fneur.2025.1534352
Post-exertional malaise in Long COVID: subjective reporting versus objective assessment
Abstract
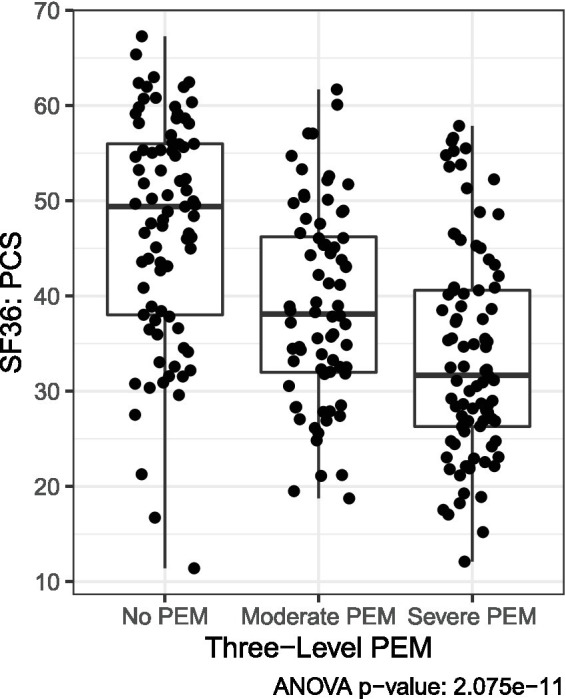
Background: Post-exertional malaise (PEM) is a central feature of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and has emerged as a prominent feature of Long COVID. The optimal clinical approach to PEM is inconclusive, and studies of the impact of exercise have yielded contradictory results.
Objective: The objective of this study was to examine PEM in Long COVID by assessing the prevalence of self-reported PEM across study cohorts and symptom responses of Long COVID patients to a standardized exercise stressor. Secondarily, Long COVID symptom responses to exercise were compared to those of ME/CFS and healthy volunteers.
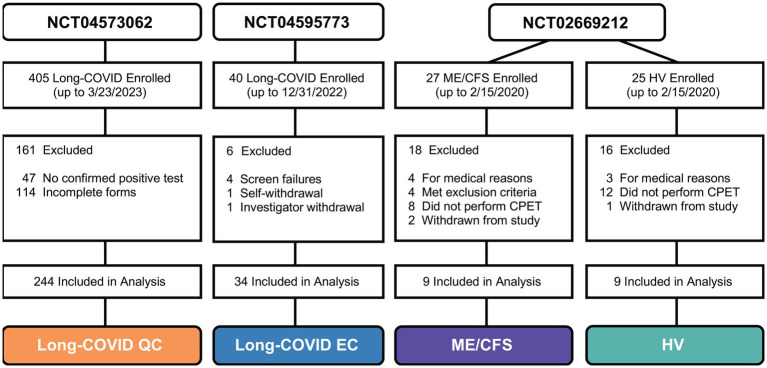
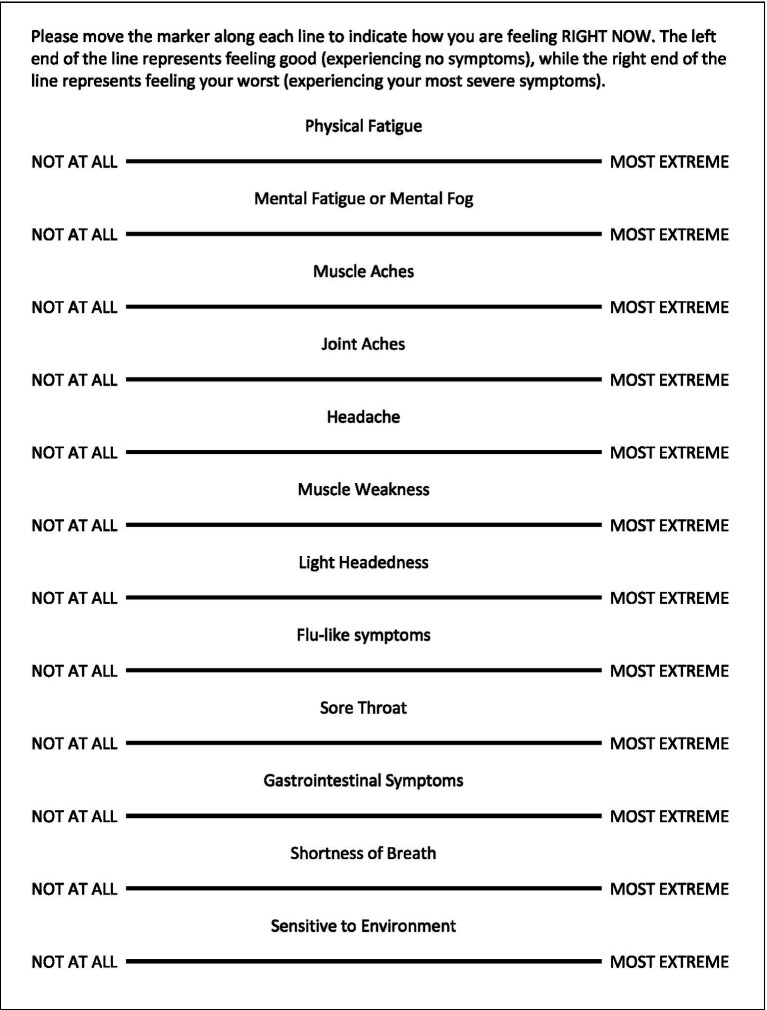
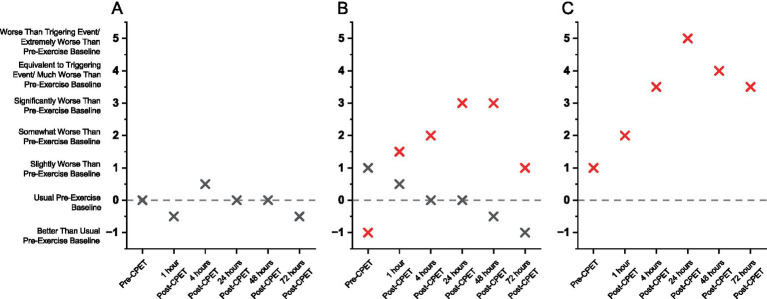
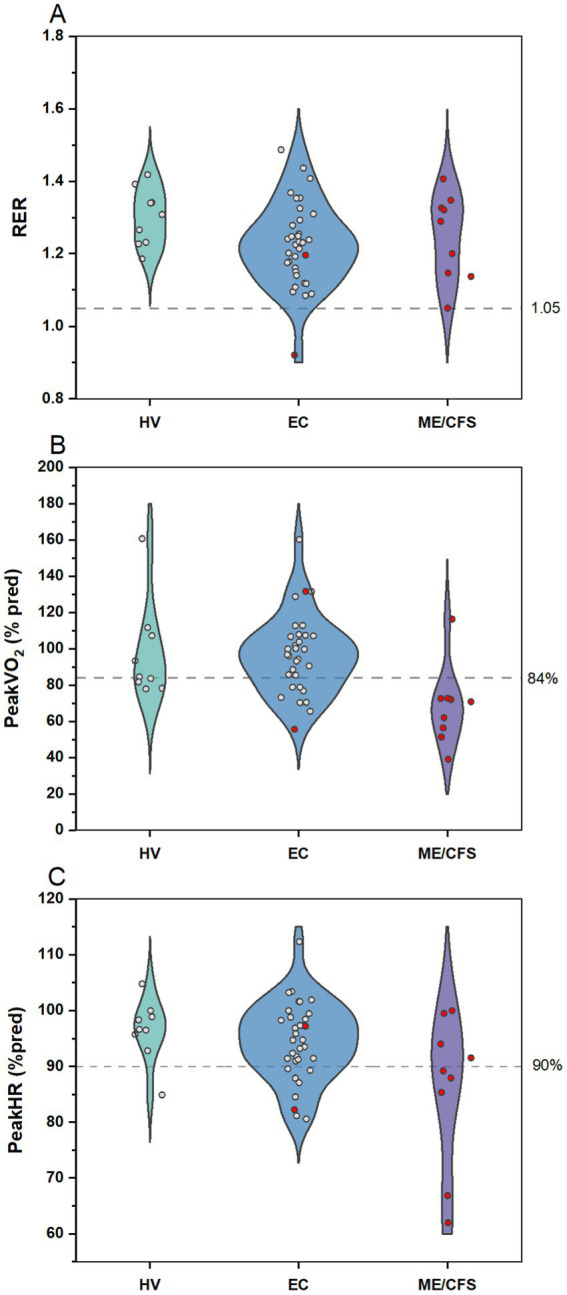
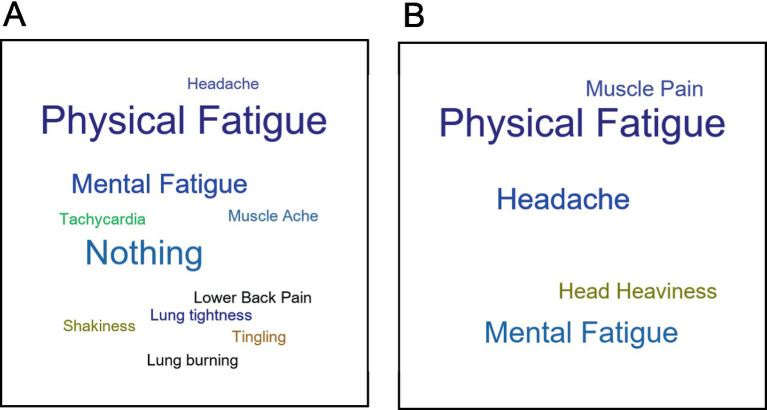
Methods: Data from three registered clinical trials comprised four cohorts in this study: Long COVID Questionnaire Cohort (QC; n = 244), Long COVID Exercise Cohort (EC; n = 34), ME/CFS cohort (n = 9), and healthy volunteers (HV; n = 9). All cohorts completed questionnaires related to physical function, fatigue, and/or PEM symptoms. EC also performed a standardized exercise test (cardiopulmonary exercise test, CPET), and the PEM response to CPET was assessed using visual analog scales and qualitative interviews (QIs) administered serially over 72 h. EC PEM measures were compared to ME/CFS and HV cohorts. A secondary analysis of QI explored positive responses to CPET among EC, ME/CFS and HV.
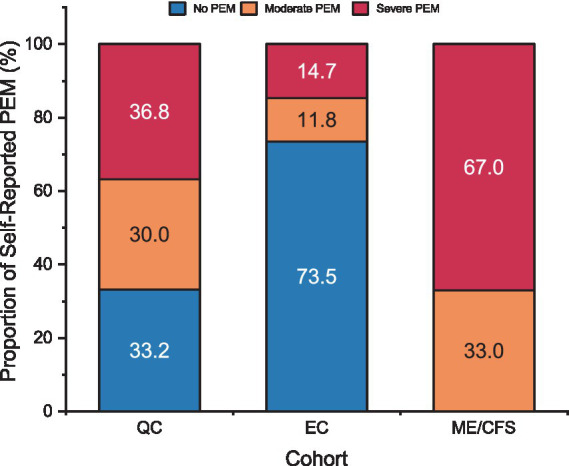
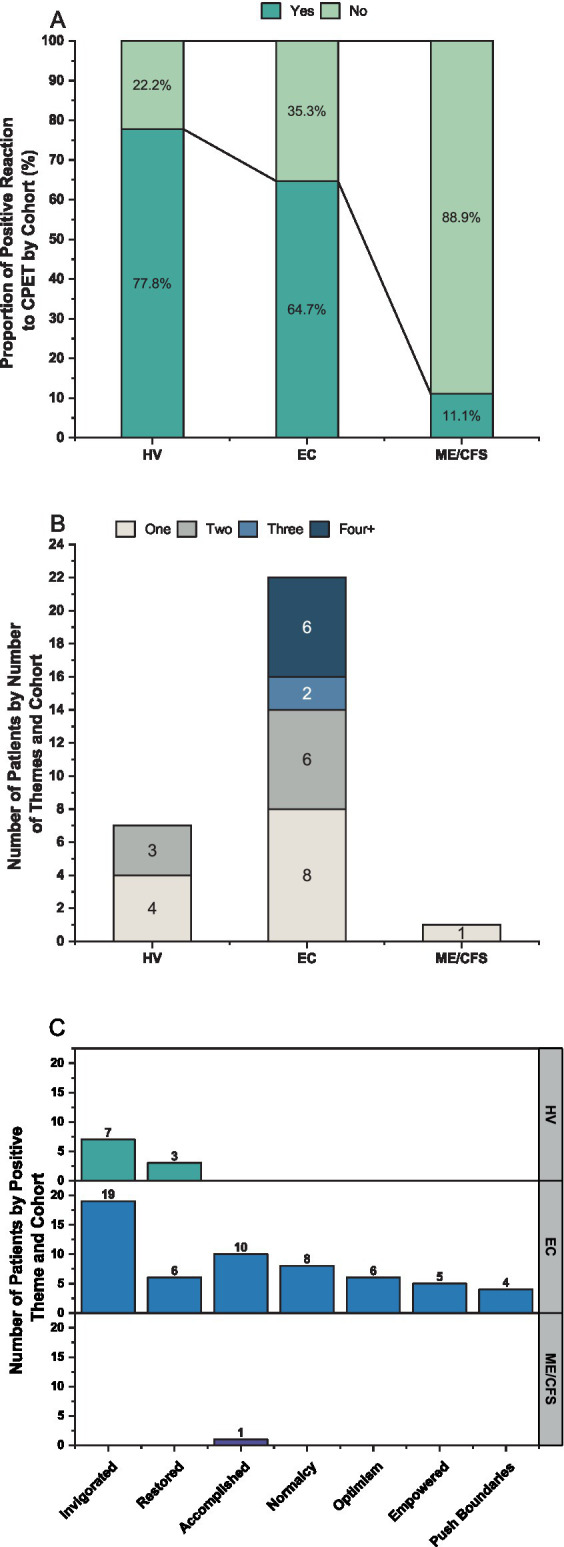
Results: Self-reported PEM was 67% in QC and estimated at 27% in EC. Only 2 of 34 EC patients (5.9%) were observed to develop PEM after a CPET. In addition, PEM responses after CPET in Long COVID were not as severe and prolonged as those assessed in ME/CFS. Twenty-two of 34 EC patients (64.7%) expressed at least one of 7 positive themes after the CPET.
Conclusion: Self-report of PEM is common in Long COVID. However, observable PEM following an exercise stressor was not frequent in this small cohort. When present, PEM descriptions during QI were less severe in Long COVID than in ME/CFS. Positive responses after an exercise stressor were common in Long COVID. Exercise testing to determine the presence of PEM may have utility for guiding clinical management of Long COVID.
Keywords: cardiopulmonary exercise test (CPET); myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS); post acute sequelae of SARS-CoV-2; post-COVID condition; post-exertional symptom exacerbation.
Copyright © 2025 Stussman, Camarillo, McCrossin, Stockman, Norato, Vetter, Ferrufino, Adedamola, Grayson, Nath, Chan, Walitt and Chin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous