

Safety and Efficacy of Robotic Hysterectomy Using an Indigenous Robotic System: A Retrospective Study
- PMID: 40337576
- PMCID: PMC12057587
- DOI: 10.7759/cureus.81832
Safety and Efficacy of Robotic Hysterectomy Using an Indigenous Robotic System: A Retrospective Study
Abstract
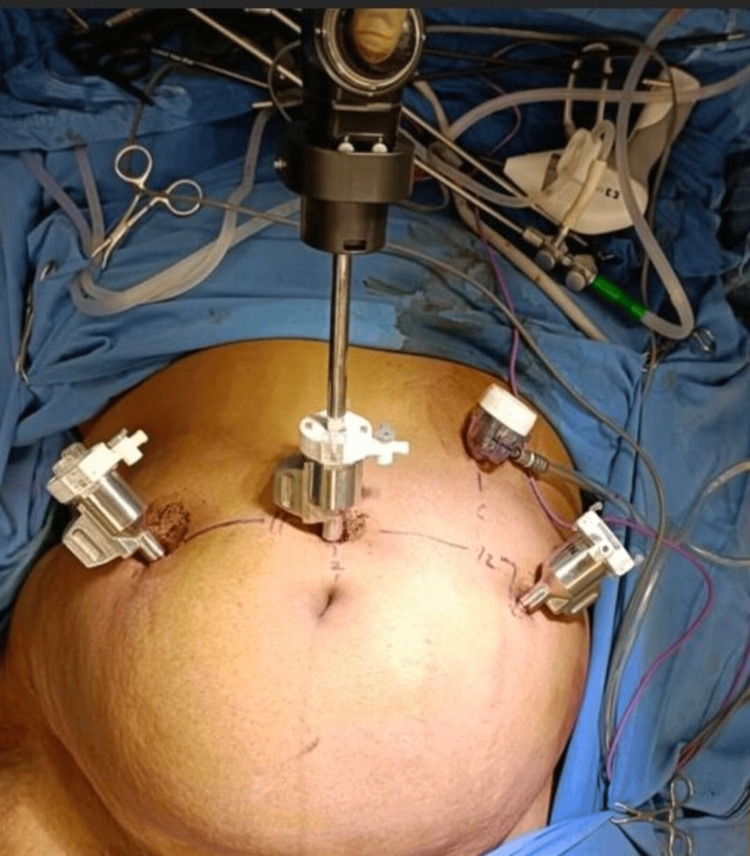
Background Minimally invasive hysterectomy approaches, including vaginal, laparoscopic, and robotic hysterectomy, offer advantages over laparotomic hysterectomy. However, vaginal hysterectomy is less feasible for patients with a large uterus, prior pelvic surgery, adnexal surgery requirements, or malignancy, making laparoscopy or robotic surgery preferable. The SSI Mantra robotic system (Sudhir Srivastava Innovations Pvt. Ltd., India) features an ergonomic open-faced console with a 32-inch 3D 4K monitor, a 23-inch 2D touch monitor for system control and DICOM applications, a head-tracking safety feature, and advanced ergonomic controls. This study evaluates the safety and efficacy of robotic hysterectomy using this indigenous system. Materials and methods From February to September 2024, 15 patients underwent robotic hysterectomy at Government Medical College, Nagpur. Patients were counseled about using the SSI Mantra robotic system and surgical risks, including possible conversion to laparotomy or robotic arm injury. The procedure followed a standard robotic port approach with accessory laparoscopic ports. Multiple surgeons performed the surgeries. The primary outcome was operative time, defined from incision start to closure. Additional data collected included patient intubation time, draping time, port placement, docking time, console time, surgical end time, patient out time, and estimated blood loss (fluid volume difference between irrigation and suction). Perioperative complications, readmissions, surgeon experience impact on operative time, conversion to laparotomy, hospital stay duration, hemoglobin drop, Visual Analogue Scale (VAS) pain scores, and intraoperative strategies (e.g., adhesiolysis, myomectomy) were analyzed. The weight of the excised uterus was also recorded. Results All 15 cases were successfully completed. The mean body mass index was 22.36 kg/m² (range: 19-25). The mean operative time (console use) was 169.41 minutes. Docking time improved from 25 minutes in the first case to five minutes by the 12th. The mean hospital stay was 4.5 days. The average uterine weight was 104.58 g (range: 25-250 g). Estimated blood loss averaged 129.16 mL (range: 30-400 mL). Vaginal cuff closure time was recorded in one case (20 minutes). The mean VAS pain score was 3.91. A hemoglobin drop occurred in four cases, but no postoperative blood transfusions were required. There were no conversions, major complications, or readmissions. Conclusions This study demonstrates that the indigenous robotic system provides enhanced ergonomics, seven degrees of freedom, ease of operation, and improved safety with a shorter learning curve for large uteri. Further studies are needed to assess postoperative and long-term outcomes.
Keywords: laparoscopy; robotic hysterectomy; safety and efficacy; ssi mantra; vas score.
Copyright © 2025, Gajbhiye et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institutional Ethics Committee of the Department of Pharmacology of Government Medical College, Nagpur, issued approval 3641EC/Pharmac/GMC/NGP. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures




References
LinkOut - more resources
Full Text Sources