

Clinical outcomes following medial meniscus posterior root repairs: A minimum of 5-year follow-up study
- PMID: 40337670
- PMCID: PMC12056713
- DOI: 10.1002/jeo2.70262
Clinical outcomes following medial meniscus posterior root repairs: A minimum of 5-year follow-up study
Abstract
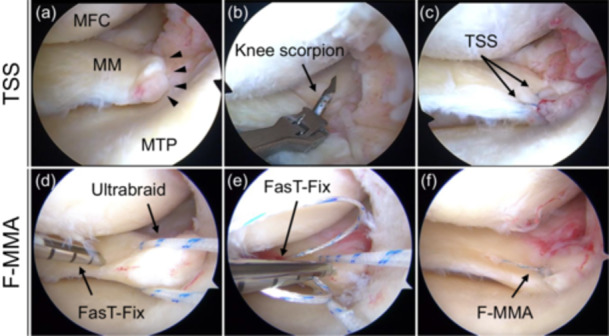
Purpose: This study assessed the clinical outcomes of the FasT-Fix dependent modified Mason-Allen suture (F-MMA) and two simple stitches (TSS) on mid-term postoperative outcomes following medial meniscus (MM) posterior root repair.
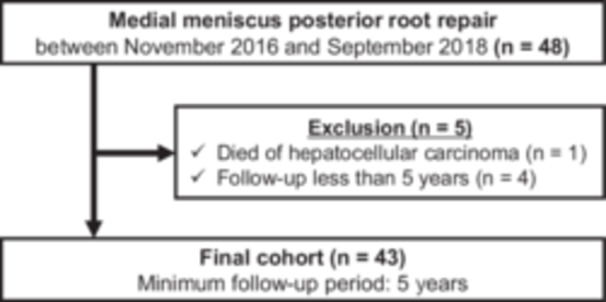
Methods: Forty-three patients who underwent transtibial pullout repair for MM posterior root tear (PRT) between November 2016 and September 2018 were initially enrolled. Patients with a femorotibial angle ≤ 180°, Kellgren-Lawrence grade of 0-2, and modified Outerbridge grade I or II cartilage lesions were included. The Lysholm, Tegner activity, International Knee Documentation Committee score, pain visual analogue scale and Knee injury and Osteoarthritis Outcome scores were assessed as clinical outcomes. Conversion surgery to knee arthroplasty was considered as the endpoint. Surgeries other than second-look arthroscopy and plate or screw removal were also recorded.
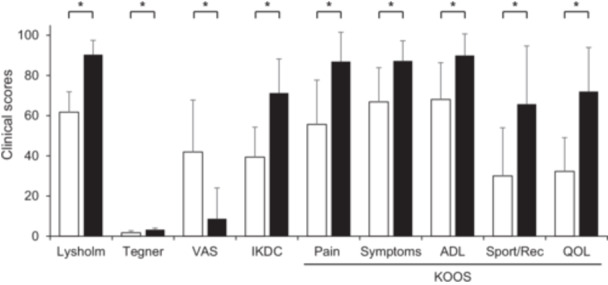
Results: The mean follow-up period was 5.9 years. All evaluated 5-year postoperative clinical outcomes were significantly improved compared to the preoperative outcomes (p < 0.001). Both the F-MMA and TSS significantly improved all clinical scores at 5 years postoperatively in patients with MMPRT, whereas the F-MMA and TSS groups showed no significant differences in the pre- and postoperative clinical scores. None of the patients required ipsilateral knee arthroplasty during the follow-up, and the survival rate after pullout repair was 100%. However, the progression of osteoarthritis could not be completely suppressed, although there were no Kellgren-Lawrence grade 4 cases. The rate of subsequent knee-related surgical treatment was 11.6% in pullout-repaired knees, including arthroscopic debridement for arthrofibrosis with a limited range of motion, an additional all-inside suture repair and partial meniscectomy.
Conclusion: Both F-MMA and TSS pullout repairs yielded satisfactory clinical outcomes in patients with MMPRT with a mean follow-up of 5.9 years, and no conversion to knee arthroplasty was required. Further follow-up is warranted to assess long-term survival rates.
Level of evidence: Level III.
Keywords: clinical outcome; medial meniscus posterior root tear; mid‐term follow‐up; survival rate; transtibial pullout repair.
© 2025 The Author(s). Journal of Experimental Orthopaedics published by John Wiley & Sons Ltd on behalf of European Society of Sports Traumatology, Knee Surgery and Arthroscopy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Ahn JH, Jeong HJ, Lee YS, Park JH, Lee JW, Park JH, et al. Comparison between conservative treatment and arthroscopic pull‐out repair of the medial meniscus root tear and analysis of prognostic factors for the determination of repair indication. Arch Orthop Trauma Surg. 2015;135:1265–1276. - PubMed
-
- Allaire R, Muriuki M, Gilbertson L, Harner CD. Biomechanical consequences of a tear of the posterior root of the medial meniscus. Similar to total meniscectomy. J Bone Joint Surg Am Vol. 2008;90:1922–1931. - PubMed
-
- Bae JH, Paik NH, Park GW, Yoon JR, Chae DJ, Kwon JH, et al. Predictive value of painful popping for a posterior root tear of the medial meniscus in middle‐aged to older Asian patients. Arthrosc J Arthrosc Rel Surg. 2013;29:545–549. - PubMed
-
- Bernard CD, Kennedy NI, Tagliero AJ, Camp CL, Saris DBF, Levy BA, et al. Medial meniscus posterior root tear treatment: a matched cohort comparison of nonoperative management, partial meniscectomy, and repair. Am J Sports Med. 2020;48:128–132. - PubMed
-
- Chung KS, Ha JK, Ra HJ, Kim JG. Preoperative varus alignment and postoperative meniscus extrusion are the main long‐term predictive factors of clinical failure of meniscal root repair. Knee Surg Sports Traumatol Arthrosc. 2021;29:4122–4130. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
