

Dynamics of interstitial lung disease following immunosuppressive treatment differ between antisynthetase syndrome and systemic sclerosis
- PMID: 40337907
- PMCID: PMC12062639
- DOI: 10.1177/17534666251336896
Dynamics of interstitial lung disease following immunosuppressive treatment differ between antisynthetase syndrome and systemic sclerosis
Abstract
Background: Interstitial lung disease (ILD) is the main clinical feature of antisynthetase syndrome (ASS). In the absence of randomized controlled trials to guide therapy, treatment strategies are often extrapolated from other diseases, mainly systemic sclerosis (SSc).
Objectives: Our aim was to evaluate the dynamics of ILD severity following immunosuppressive treatment (IST) in ASS compared to SSc.
Design: A multicenter retrospective observational study.
Methods: ASS (n = 22) and SSc (n = 32) subjects with ILD were included in the registries of three medical centers. All patients received ISTs. We analyzed changes in forced vital capacity (FVC) and diffusion capacity for carbon monoxide corrected for hemoglobin (DLCOc) after treatment initiation using linear mixed-effects models. Changes in high-resolution chest CT scans were analyzed by a radiologist blinded to clinical data.
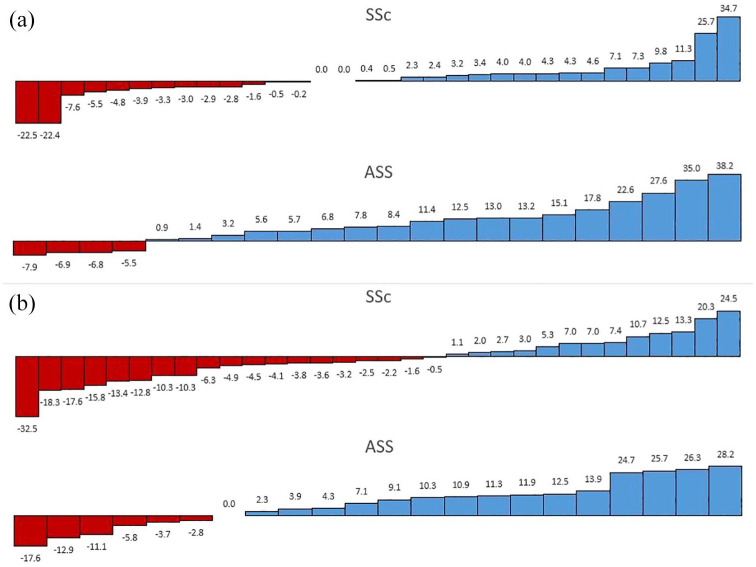
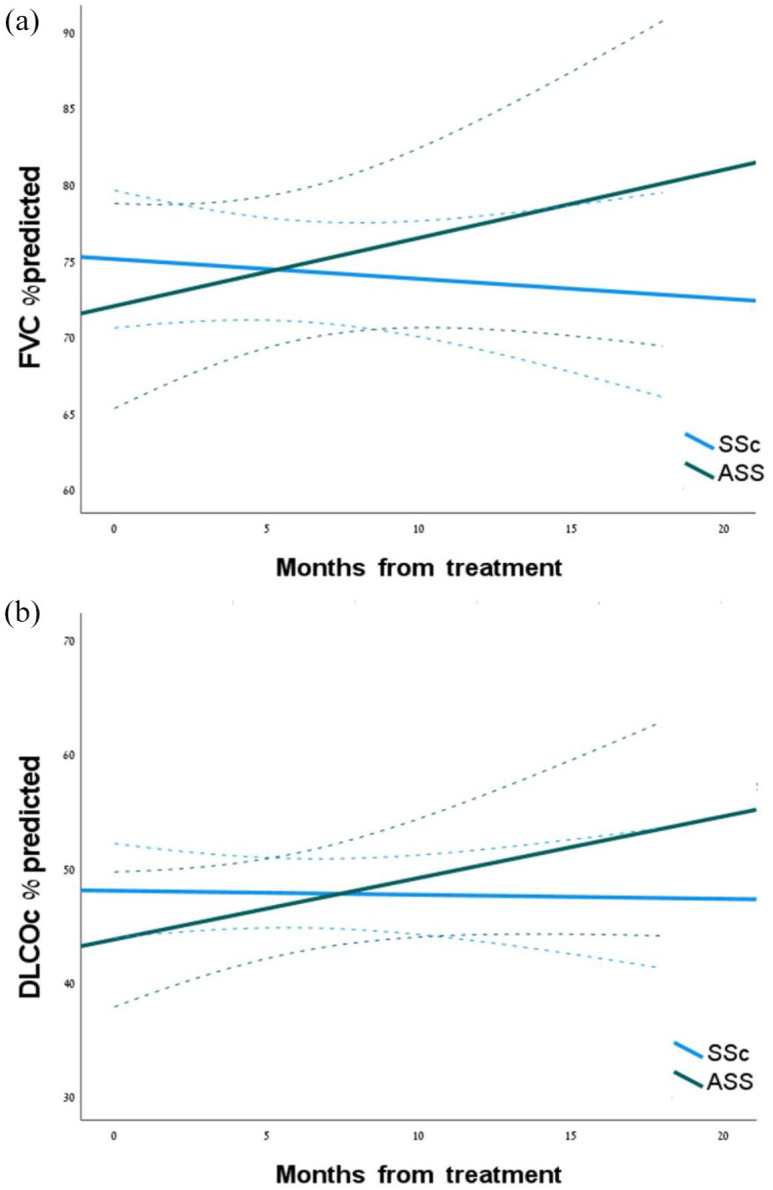
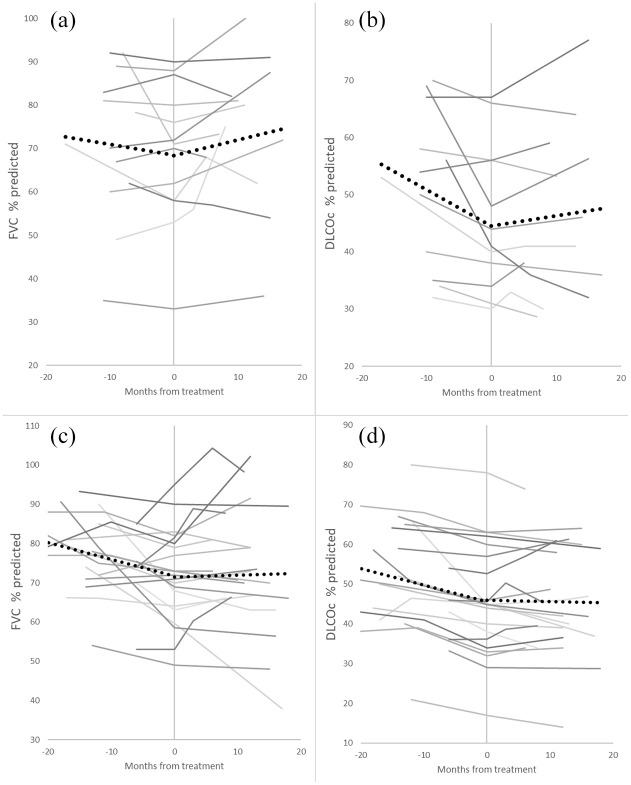
Results: The median (interquartile range) age was 66 (59-71), 72% were females, and 81% of IST included mycophenolate mofetil (MMF). Baseline demographics, comorbidities, and pulmonary functions were similar between the groups. Among the ASS group, the mixed-effects models showed significant improvements in FVC% (F = 11.3, p < 0.01) and DLCOc% (F = 7.1, p = 0.015) after treatment initiation over time, while in the SSc group, there were no significant changes in FVC% (F = 0.4, p = 0.551) and DLCOc% (F = 0.8, p = 0.384). Changes in FVC% and DLCOc% were higher in the ASS group compared with SSc (p = 0.017 and p < 0.01, respectively), which persisted after adjustment to steroid use and in a sub-analysis of patients with serial pre- and post-IST pulmonary functions. Both groups had improved total CT scores after IST, without changes in other radiologic scores.
Conclusion: Immunosuppressive treatment, mostly with MMF, was associated with significant improvement of FVC% and DLCOc% in ASS, compared to their stabilization only in SSc. This should encourage future randomized controlled studies of MMF in ASS patients.
Keywords: high resolution CT; lung functions; mycophenolate mofetil; pulmonary fibrosis; steroids.
Plain language summary
How interstitial lung disease progresses after immunosuppressive treatment in antisynthetase syndrome vs. systemic sclerosisAntisynthetase syndrome (ASS) is a rare autoimmune disease that affects the muscles, joints and lungs. Systemic sclerosis (SSc) is also a less rare autoimmune disease that causes scarring of the skin and the lungs, for which there is more abundant clinical trial evidence to support treatment. For both diseases, immunosuppressive treatments are required, which are treatments that lower the activity of the body’s immune system. As there are no official treatment guidelines for managing ASS lung disease, doctors often rely on established treatments for SSc lung disease. For this reason, our aim was to assess how lung disease responds to immunosuppressive treatment in ASS compared to SSc. We looked back at data of 54 patients from three medical center. 22 patients had ASS lung disease and 32 patients had SSc lung disease, all treated with immunosuppressive therapy. We found that lung function has significantly improved in the ASS group after treatment. This improvement was greater than that observed in the SSc group. CT scans, which depict the changes in the relevant lung disease, showed improvements in both groups. Additionally, we identified markers that may help predict how patients with ASS will respond to immunosuppressive treatments. In summary, we found major improvements of ASS lung disease compared to SSc after starting immunosuppressive therapy, supporting the need for additional high-quality research that focus on ASS.
Figures
References
-
- Connors GR, Christopher-Stine L, Oddis CV, et al.. Interstitial lung disease associated with the idiopathic inflammatory myopathies: what progress has been made in the past 35 years? Chest 2010; 138(6): 1464–1474. - PubMed
-
- Bahmer T, Romagnoli M, Girelli F, et al.. The use of auto-antibody testing in the evaluation of interstitial lung disease (ILD)—a practical approach for the pulmonologist. Respir Med 2016; 113: 80–92. - PubMed
-
- Kalluri M, Oddis CV. Pulmonary Manifestations of the Idiopathic Inflammatory Myopathies. Clin Chest Med 2010; 31(3): 501–512. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
