

Regional variation in traumatic brain injury patterns, management and mortality: a nationwide Swedish cohort study
- PMID: 40338360
- PMCID: PMC12062049
- DOI: 10.1007/s00701-025-06557-w
Regional variation in traumatic brain injury patterns, management and mortality: a nationwide Swedish cohort study
Abstract
Background: Sweden covers a large land area, but is sparsely populated. The country is divided into six heterogenous healthcare regions, each with different geographic conditions and referral patterns when it comes to traumatic brain injury (TBI). This study aimed to explore the variation in demography, injury patterns, care pathways, management, and mortality (30 d) for TBI patients within the country.
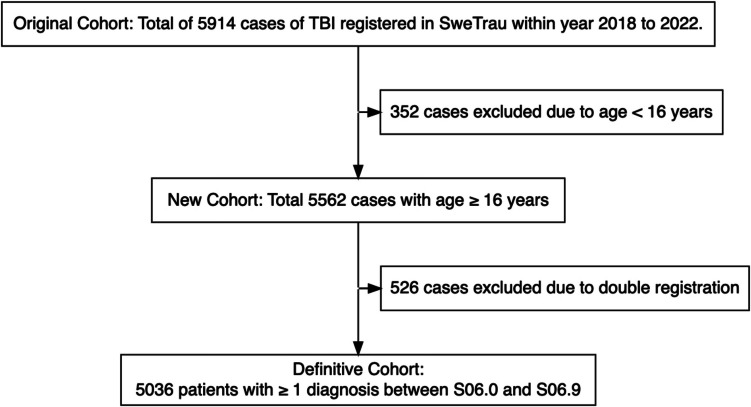
Methods: A nationwide, observational study, using data from the Swedish Trauma Registry (SweTrau) between 2018-2022, was performed. A total of 5036 TBI patients were included. Data on demography, admission status (through Glasgow Coma Scale [GCS] value at arrival at first managing hospital), injury-related variables, and mortality (30 d) were evaluated.
Results: The median age was 65 years (interquartile range 46-78), and the majority of patients were male, had sustained fall-related injuries, and were conscious upon admission. Slight, but significant differences (p < 0.05) existed among the regions in these variables. In multivariate logistic regression models, the healthcare region (p < 0.05) was independently associated with patient referral to a university hospital (as compared to care at a local hospital alone), craniotomy rate, and receiving an intracranial pressure-monitoring device, after adjustment for demographic and injury variables. In similar regressions regarding mortality, specific healthcare regions (p < 0.05) were independently associated with said outcome.
Conclusions: The study highlights, from a systems-level perspective, that there was a significant variation in care pathways and management among the six healthcare regions in Sweden, which might have impacted on clinical outcome. These findings call for more granular studies to understand which aspects of patient management that were particularly beneficial or detrimental for patient survival and recovery.
Keywords: Craniotomy; Epidemiology; Neurointensive care; Outcome; Traumatic brain injury.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no competing interests. Human ethics and consent to participate: The study was approved by the Swedish Ethical Review Authority (Dnr 2023–07084-01) for the use of SweTrau registry data. Informed consent was not required; however, participants had the opportunity to opt out of data registration and request the removal of their registered data from SweTrau.
Figures

Similar articles
-
Hyperbaric oxygen therapy for the adjunctive treatment of traumatic brain injury.Cochrane Database Syst Rev. 2012 Dec 12;12(12):CD004609. doi: 10.1002/14651858.CD004609.pub3. Cochrane Database Syst Rev. 2012. PMID: 23235612 Free PMC article.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Elevation of the head during intensive care management in people with severe traumatic brain injury.Cochrane Database Syst Rev. 2017 Dec 28;12(12):CD009986. doi: 10.1002/14651858.CD009986.pub2. Cochrane Database Syst Rev. 2017. PMID: 29283434 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
Diagnostic management strategies for adults and children with minor head injury: a systematic review and an economic evaluation.Health Technol Assess. 2011 Aug;15(27):1-202. doi: 10.3310/hta15270. Health Technol Assess. 2011. PMID: 21806873 Free PMC article.
References
-
- Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW, Servadei F, Walters BC, Wilberger JE (2006) Guidelines for the surgical management of traumatic brain injury author group: Acknowledgments. Neurosurgery 58(3):S2 - PubMed
-
- Carney N, Totten AM, O’Reilly C et al (2017) Guidelines for the management of severe traumatic brain injury fourth edition. Neurosurg 80(1):6 - PubMed
-
- Elf K, Nilsson P, Enblad P (2002) Outcome after traumatic brain injury improved by an organized secondary insult program and standardized neurointensive care. Crit Care Med 30(9):2129–2134 - PubMed
-
- Fischerström A, Nyholm L, Lewén A, Enblad P (2014) Acute neurosurgery for traumatic brain injury by general surgeons in Swedish county hospitals: A regional study. Acta Neurochir 156(1):177–185 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
