

Neuromodulation in Chronic Migraine: Evidence and Recommendations from the GRADE Framework
- PMID: 40338487
- PMCID: PMC12182506
- DOI: 10.1007/s12325-025-03206-7
Neuromodulation in Chronic Migraine: Evidence and Recommendations from the GRADE Framework
Abstract
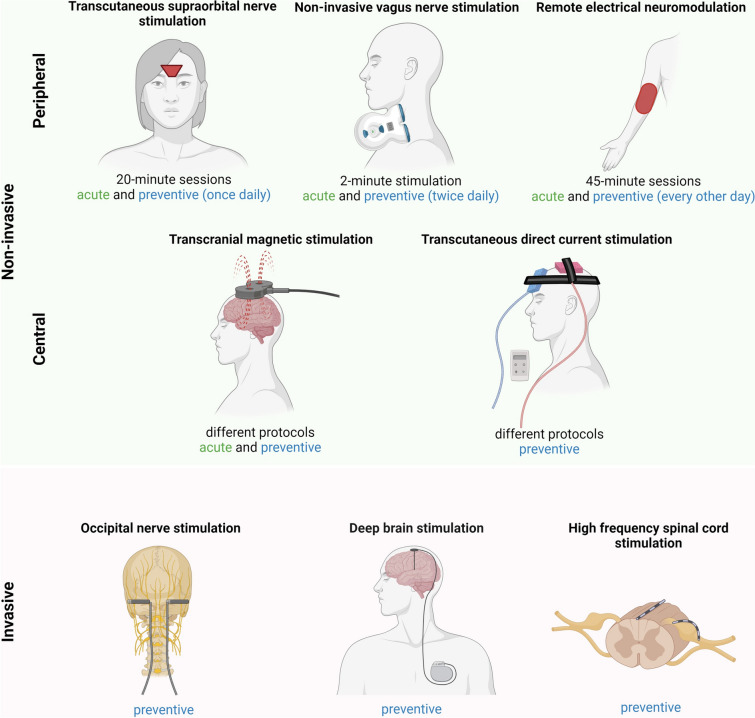
Chronic migraine (CM) affects approximately 2% of the general population and is defined by the persistence of migraine symptoms for at least 15 days per month for at least 3 months. CM is often refractory to common drug treatments and is associated with a significant burden in functions of daily life during ictal phases, productivity loss, and direct costs. Modulation of pain is considered pivotal to reduce its impact and to improve the quality of life among patients with CM. In recent years, neuromodulation in CM has received growing attention; however, there remains no consensus regarding the effectiveness and safety of these procedures. Previous invasive methods such as occipital nerve neurolysis and interruption of the trigeminal dorsal root are not indicated due to high rates of relapsing pain and frequent procedural complications. Although emerging neuromodulation methods, both noninvasive, such as vagus nerve stimulation (VNS), transcranial magnetic stimulation (TMS), remote electrical neuromodulation (REM), and invasive, such as deep brain stimulation (DBS), occipital nerve stimulation (ONS), and high-frequency 10-Hz spinal cord stimulation (HF-10 SNS) have demonstrated promising outcomes in early clinical trials, their use has yet to be integrated into routine clinical practice. In this review, study evidence and strength of recommendations are assessed by the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system. Other conditions such as therapeutic risk/benefit, direct and indirect costs, use of resources, and patient/clinician preferences are also evaluated.
Keywords: GRADE; Migraine; Neuromodulation; Remote electrical neuromodulation; Stimulation; Vagus nerve.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interests: Claudio Tana is member of Editorial Board: The Journal of Headache and Pain and Editor of the Primary Care Section of Annals of Medicine. David Garcia Azorin is member of Editorial Board: The Journal of Headache and Pain, and has received research funding from the Regional Health Administration (Gerencia Regional de Salud SACYL) in Castilla y Leon, Spain. Speaker/travel grants/ clinical trials from Teva, Abbvie, Amgen, Eli Lilly, Lundbeck, Novartis, Pfizer and Biohaven. Bianca Raffaelli is member of Editorial Board: The Journal of Headache and Pain; reports personal fees from AbbVie, Eli Lilly, Lundbeck, Novartis, Organon, Perfood and Teva for participating in advisory boards and/or speaker activities as well as research funding from Lundbeck, Novartis, Else Kröner-Fresenius-Stiftung, German Research Foundation and German Migraine and Headache Society. Mira Pauline Fitzek reports personal fees from Teva, Novartis. Marta Waliszewska-Prosół is member of Editorial Board: The Journal of Headache and Pain; reports personal fees from AbbVie, Pfizer, Polpharma and Teva for speaker activities. Sonia Quintas has received honoraria from Lilly, Novartis, Exeltis, UCB Pharma, Bial and Altermedica. Paolo Martelletti is the Editor-in-Chief of The Journal of Headache and Pain and of SN Comprehensive Clinical Medicine. Ethical Approval: This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
